
Brain-Based Views on Psychotherapy Integration: Clinical Biopsychology

❝Despite the advances in understanding the link between psychotherapy and the brain, many psychotherapists lack the knowledge base to critically evaluate brain-related studies and how this information relates to different psychotherapy approaches and their integration.❞
There has been a growing interest in the brain as it relates to psychotherapy over the past 20 years. Concepts such as “mirror neurons” and “memory reconsolidation” have captured the field’s attention. The role of the amygdala in fear conditioning as related to trauma and subcortical emotional memory storage appear as common themes. Despite this interest, many psychotherapists lack the knowledge base to critically evaluate brain-related studies and how this information relates to different psychotherapy approaches and their integration.
To date, I believe the highest level of integration of the three traditional psychotherapy orientations (i.e., psychodynamic, humanisitic/experiential, and behavioral/cognitive-behavioral) has involved conceptualizing cases with one orientation, but “borrowing” treatment techniques from other areas. If an accurate description of how the brain operates can be provided, it logically follows that a higher level of integration can be accomplished. In this regard it should become apparent that treatments derived from each orientation have a basis for why they can be effective in some cases, but it should also be apparent how the approaches are connected and why other techniques may provide additional benefit. I am sure most of you recall the story of the three blind men each touching different locations (i.e., trunk, body, or tail) on an elephant and describing what was felt. Although being accurate, the descriptions appear quite different and irreconcilable. If one can get the full visual view of the elephant, it becomes obvious the various parts are connected in a logical fashion.
Looking for evidence-based support? Find a qualified psychologist near you through TherapyRoute.
Find a PsychologistTo facilitate an understanding of the more technical aspects of a brain model I term the Dimensional Systems Model and its relationship to a psychotherapy orientation I call Clinical Biopsychology, I want to give some general comments. First, all nervous system activities work by synaptic connections. At the synapse a neurotransmitter is released which can lead to excitation or inhibition of the connecting neurons. In the cortex, glutamate is the excitatory neurotransmitter while GABA is inhibitory, a distinction taken up in a proposed new comprehensive model of consciousness and emotion. If there are no connections, then two areas cannot communicate directly. This is critical in an understanding of “conscious” versus “unconscious” processing and responses.
The brain requires an accurate representation of both external and internal stimuli. Thus, sensory information that arrives at the cerebral cortex is as an accurate reflection of those stimuli, followed by the processing of the information which allows meaningful action. The same cortical areas involved in the original processing of information are the same areas reactivated when the memory is recalled. This means that all the sensory memories, including those emotional in nature, involve direct connections at the cortical level, not the subcortical level.
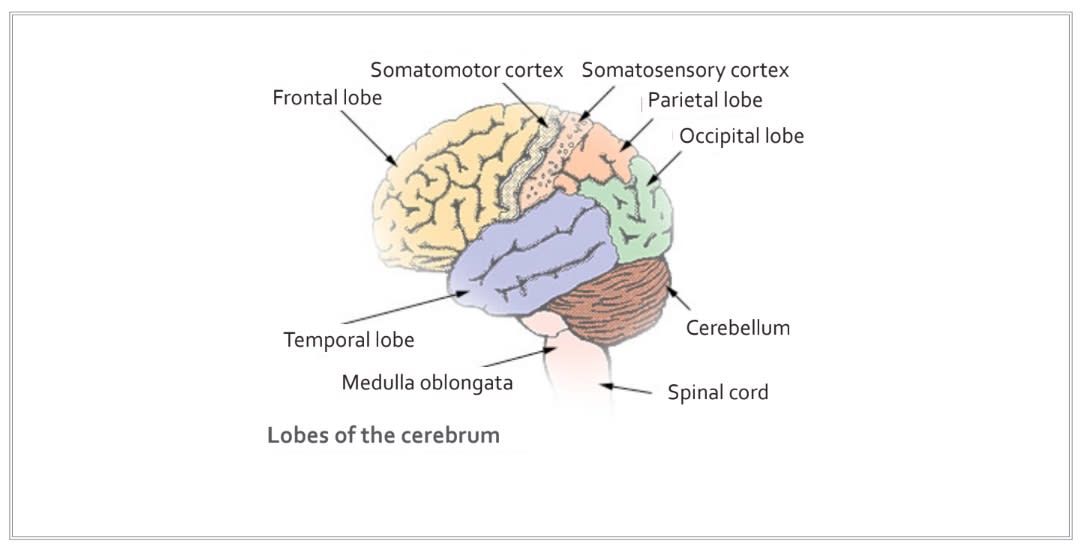
In relation to the cerebral cortex, I have suggested the binary unit (bit) for all information processing and memory storage is the cortical column. For the purposes of this article, just think about the fact that each column is a group of a few thousand neurons that represents specific information. When sensory receptive columns activate, they in turn send neuronal information outward and where the outgoing activity of one or more columns crosses, a new column is formed. That new column now represents all the information of the columns that sent information to it. This leads to circuits of columns (i.e., a memory) such that when the same sensory information arrives at the cortex, the same circuit of receptive columns activates. With the formation of a new receptive column (located in the parietal, temporal, or occipital lobes which are considered the “posterior lobes” since they are behind the central sulcus), that column also projects to the frontal lobe where an action column forms. The action column can in turn lead to activation of other action columns which become behavioral responses. This means that all memory formation is the same throughout the cortex and perceived differences in types of memory (e.g., visual versus auditory) are a function of which columns are in the circuit. This is similar to two simple electrical circuits, both of which have a battery and switch, but one has a light bulb and the other a bell. The basic circuits are the same, but each leads to a different result when activated.
Another point is that a primary goal is to activate positive emotions and deactivate negative ones. This is consistent with the psychodynamic concept of the pleasure principle, as well as positive and negative reward in behavioral formulations. It is important to store information on what situations/factors lead to emotional reactions, which means that the stronger the emotional response, the more enhanced will be the association memory. When emotional memories are activated in the cortex, the columns connect to subcortical structures (e.g., amygdalae, mesolimbic dopaminergic pathway) which in turn activate the physiological and motivational aspects of emotions. Since brain structures are paired, then both the right and left cortices have their own respective subcortical structures. This means each hemisphere is capable of producing both positive and negative emotional reactions.
In addition to the well known distinction of simultaneous right and left cortical activity, there are also multiple streams (i.e., circuits of columns) of information processing that occur in the same hemisphere (e.g., autobiographical information is stored in the medial cortex while external information is stored laterally). Whichever information streams are the most relevant to an ongoing situation are the onesleading to action associated with attention and behavioral responses. Since these processes occur in fractions of seconds and have been present for one’s lifetime it gives us the subjective impression that in most circumstances the “mind” is a uniform whole. In reality, whichever circuits can most effectively analyze and respond to a given situation are the ones that assume control. As will be explained, this means that there is often a lack of accurate verbal awareness as to why one’s own actions occur.
The right cortex processes information in a global manner which allows it to be relatively faster in processing speed than the left, though the right side has less capacity for fine detail in both analysis and response. Global processing results from relatively fewer columns (compared to the left cortex) in the circuit from the time of sensory input to behavioral response on the right side. Of particular relevance to psychotherapy is the fact that interpersonal interactions rely heavily on non-detailed voice intonations and facial expressions that the right cortex is best suited to handle. This means that the non-detailed emotional and interpersonal sensory and motor memories are stored in the right hemisphere. Thus, many of the sights, sounds, and touches associated with negative emotional memories, including traumatic ones, are stored in the right posterior lobes. The right cortex is responsible for our interpersonal “native emotional language” (analogous to the native spoken language of the left hemisphere) leading to our “personality” characteristics. The left cortex involves analytical processing, since it has many more columns involved in its circuits. This means it can handle much more detail in processing, response, and memory storage.
With those basic points made, in relation to psychotherapy I will discuss several important concepts to demonstrate how a clinical biopsychological perspective can provide insight. The discussion is by no means exhaustive of all the points, just representative of how applying the model can lead to psychotherapy integration. The interested readers are referred to my prior articles (Moss, 2006, 2007, 2010, 2013a, 2013b; Moss et al., 2012) and treatment manual (Moss, 2001) for more detailed accounts.
The verbal interpreter and “consciousness”
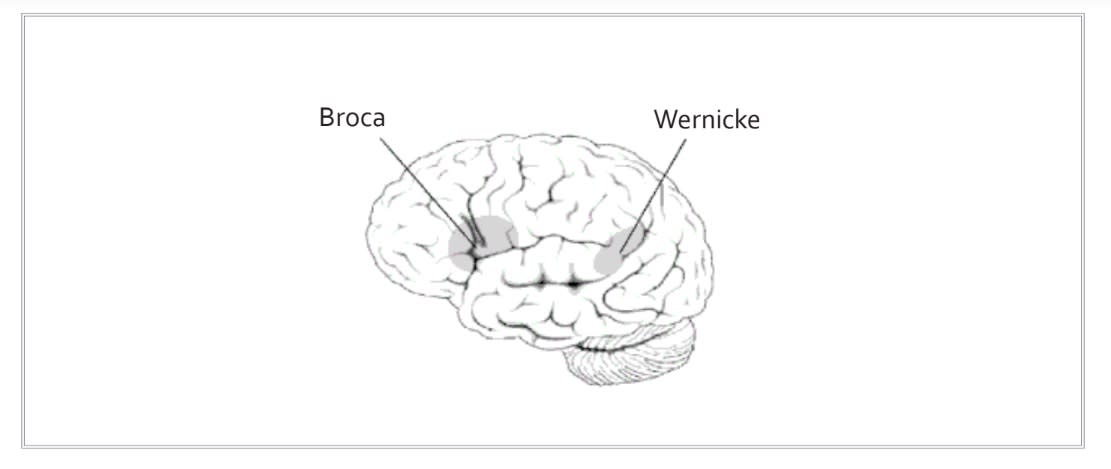
I originally (Moss, 2001) referred to the left hemisphere being involved with all verbal-thinking, including one’s internal verbal dialogue. Gazzaniga (2002) similarly described the “interpreter” of the left hemisphere. I now use the term verbal interpreter to refer to the ventral lateral frontal region which includes “Broca’s area.” Although the receptive language memories are located in the posterior lobes, the columns allowing us to actively use language are in the frontal lobe. If accurate, our internal verbal dialogue, which has often been considered synonymous with “consciousness” or self-awareness, involves only a limited area of the left frontal cortex. Therefore, if there are no direct cortical connections to allow the verbal interpreter to be aware of specific cortical activity located elsewhere, the other activity is “unconscious” relative to verbal awareness.
A major question is what is connected to the verbal interpreter’s location? Obviously, left cortical functions are the most likely to be accessible by the interpreter, particularly in the lateral cortex. Medially located internal/self-referential processing and memories of the left hemisphere are less likely to connect. This is based on the expectation that medial receptive columns are connected to their respective medial frontal columns. If medial frontal columns can lead to a meaningful or effective response, there is no need to have activation in the region of the verbal interpreter. For example, if the mesolimbic dopaminergic pathway activates, this theoretically leads to the involvement of the action columns which are medially located in the cortex. The result is a general activation in behavior (i.e., appetitive reward system) associated with positive affect (euphoria/ excitement) that has been called the SEEKING system by Alcaro and Panksepp (2011). In this case there is a desire to seek some goal although the specific stimulus (e.g., favorite food versus sex versus alcohol) sought may vary depending on the internal or external stimulus leading to the initial activation of the dopaminergic system. In this case one’s verbal interpreter may be unaware of the factors leading to the activated state, although it may be aware of a desire or urge based on bodily sensory changes or perceived images originating in the right cortex.
In relation to right cortical connections to the verbal interpreter, these are very limited. It appears that frontal connections from one hemisphere connect only to the corresponding location of the opposing hemisphere. The same is true of the posterior cortical regions. This suggests that most right hemisphere processing is not directly connected with the verbal interpreter. The result is that there is inaccurate awareness of, and an inability to control, right posterior hemisphere activities by the verbal interpreter.
Psychotherapy is primarily dependent on language as the means to facilitate change. This means the left hemisphere is primarily involved in ongoing aspects of verbal interaction. However, the right hemisphere can become involved in several ways during conversations. If visual images are evoked, such as with metaphor and analogies, this involves the frontal action and posterior sensory columns on the right side. Additionally, verbally initiated experiential techniques (e.g., role plays and role reversals; chair techniques; psychodrama) engage the right cortex. However, one key point relates to a basic tenet of cognitive-behavioral approaches, which is that the way we talk to ourselves or interpret situations will determine our emotional reactions. This is true only of the left hemisphere’s reactions but not the right hemisphere. This is the reason that many experiential therapists have emphasized the need to elicit affect (i.e., right cortex) to address affect-laden memories. In other words, both the cognitive-behavioral and experiential therapists are right, but both have many times unknowingly supported treating only half the brain. In my view, both the left and right hemispheres need to be addressed in comprehensive psychotherapy.
Process variables, mindfulness, and interhemispheric congruence
The concept of interhemispheric congruence simply means that both hemispheres are in concert in relation to both reception and action. In other words, there is no conflict in perception and response. This is present most of the time and in most aspects of our lives. If engaged in a task such as hitting a drum with drumsticks, there is smooth inter-hemispheric coordination from one hand to the other while listening to the rhythm. In this example the motor planning areas in each frontal lobe shift control from side to side, relying on the posterior columns’ sensory feedback. However, we are all aware of the conflict that occurs when we verbally think one way but feel quite differently about some matter. In such cases we verbally think it is illogical to feel what we do, but are unable to change the feelings. This is an example of interhemispheric incongruence.
Theoretically speaking, the source of most such conflict involves the verbal interpreter’s schema of what should be felt emotionally being discrepant from the emotional perception based on activation of the right posterior sensory memories and the associated affect expressed by the right frontal lobe. Since there are no direct connections between the left frontal and right posterior cortical regions, there is no manner for the verbal interpreter to either perceive the specific right posterior cortical memories being activated or control those memories. Since the non-verbal emotional action columns of the right frontal lobe are in conflict with the verbal interpreter, there will be inhibition by each side of the input from the opposing frontal cortex. This conflict of the action columns of each hemisphere is perceived as an internal conflict with increased tension and anxiety. On the other hand, if the verbal interpreter is either disengaged or its interpretive schema is in line with the right cortical processing, the perception is one of internal peace. There a number of ways different psychotherapy orientations approach the creation of hemispheric congruence.
I find it helpful to imagine that, in any interaction between two individuals, including psychotherapy, there are four separate minds present. This refers to the right and left cortical hemispheres of both individuals. Left hemisphere therapy skills are easily learned via language, with the result being these can be presented to clients’ left hemispheres efficiently. However, a therapist’s own right posterior cortical emotional processing and right frontally-based expression are completely different stories. For anyone who has been involved in clinical training of graduate students, there should be no doubt that some students appear to have “natural” abilities as therapists while others are woefully deficient in non-verbal therapeutic skills. These distinctions are the result of right cortical functions. Clinicians who are involved in full time practice will hopefully find their own right cortices learn based on what works with clients and improve their own non-verbal perception and expression, frequently with no verbal awareness of the right cortical learning. This is a basis for one argument practicing clinicians have made about using only manualized, evidence-based therapies. Written information in manuals can address only the therapist’s left hemisphere and has no direct impact on psychotherapeutic skills of the right cortex.
The process variables of warmth, genuineness, and empathy described by Rogers (1957) are important for the most effective therapy regardless of orientation. Warmth is primarily processed in the client’s right hemisphere. Non-detailed therapist behaviors such as voice intonation, body position, facial expressions, and eye contact are keys in conveying warmth and acceptance. The therapist’s right frontal lobe action columns are those that allow therapeutic expression of warmth. In genuineness, therapists have hemispheric congruence such that their own verbal interpreters are in line with their own right hemisphere processing. This allows the communication of truthful and consistent verbal and emotional messages to the client, both based on verbal content and with the heartfelt aspect of the accuracy being conveyed by the therapist’s non-verbal behaviors. The result for the client is consistency in the processing of the receptive information in both the right and left posterior cortical columns followed by the associated frontal columns being activated. Since the client’s frontal columns of both hemispheres have consistency, the client will experience minimal conflict. In relation to the process variable of empathy, the accurate verbal labeling or acknowledgement of the client’s emotional state results in alignment of the client’s left verbal posterior processing and the right posterior processing. In this case the left posterior column activation of the connected frontal columns aligns the left frontal verbal interpreter with the affective right frontal processing. In both empathy and genuineness, there is less inhibition between the frontal lobes in the client’s brain. This is perceived by the client as decreased internal conflict and increased peace. In total, the presence of these process variables creates the security and hemispheric congruence in therapy allowing the client to most effectively address important issues.
Mindfulness techniques focus on experiencing in the present with the absence of any value judgments tied to ongoing experiences. The direction to avoid judgment of experiences gives a new schema to the verbal interpreter which, if successfully used, decreases any existing conflicts of prior verbal schemas with right hemisphere-based emotional reactions. In addition, attention is focused on experiences (e.g., focused on the sensations of breathing) mediated by frontal columns other than those of the verbal interpreter. Disengagement of the verbal interpreter necessarily removes conflicts. When a person is practicing this new approach, there are new frontal action columns formed in both hemispheres which, when well consolidated, allow the client to use the technique effectively in managing maladaptive urges and emotional reactions. Other schemas are often taught to the verbal interpreter, such as “acceptance” of one’s emotional state/reactions without attempts to necessarily modify/change the conditions perceived as leading to the state or reactions. In all cases, new frontal cortical columns are formed based on the newly learned skills.
Clinical biopsychology case conceptualization
Providing a comprehensive and comprehensible conceptualization to a client is important for several reasons. First, it informs the client that the therapist has taken the information from the initial assessment to formulate an understanding of why the current problems exist. The explanation provides the client’s verbal interpreter with a new schema which, in turn, increases inter- hemispheric congruence, allowing clients to feel more at ease. The conceptualization is also important in letting the client know there is a plan on the manner the problems will be addressed. To some degree, this allows the client to know what his/her role will be in treatment. Additionally, clients who believe they can be helped are much more likely to return for the next therapy session.
Within the clinical biopsychological approach, assessment is completed in a single session. This is accomplished since the therapist is aware of the critical factors to be assessed and asks the basic questions to gather the required information. At the beginning of the session the client is told that a broad range of questions will be asked, but only limited details will collected. A client who understands this allows the most efficient means to receive an explanation and initiate formal treatment is typically very willing to comply. In reality, I believe this also communicates to the client that the therapist is expert and knowledgeable. The conceptualization is presented to the client in the second session and treatment is started in the third session.
The clinical biopsychological conceptualization begins with an explanation of the general physiological characteristics associated with negative emotional states and why these occur. This is consistent with biopsychosocial explanations of the role psychological factors play in various disorders (e.g., cardiovascular disease, chronic pain), as well as the autonomic characteristics of panic attacks. Unlike biopsychosocial formulations, there is an explanation that the physical symptoms often activate based on negative emotional memories housed in the right posterior cortex with no “conscious” verbal awareness. This happens in the course of the general explanation of cortical design and memory storage. The next aspect explained is the fact that that negative mood states can result from one or a combination of three sources: ongoing factors (e.g., argument, pain); activation of negative emotional memories (e.g., trauma); and inability to activate previously stored positive emotional memories (e.g., relationship loss, abstinence from a pleasurable activity or substance). The client’s historical information is used in the description of the developmental history of the current problems, with the conclusion of the session involving a brief description of the treatments recommended to address each of the identified areas.
Native emotional language, attachment, and personality
Since both hemispheres are similarly designed in terms of columnar processing patterns, it follows that what is true of one side of the cortex is true of the other side. Since the verbal interpreter is aware of left hemisphere language functions, there is a tendency for therapists and clients alike to see those functions as natural. For example, we verbally learn new concepts and incorporate these with our pre-existing views and concepts tied to many things in our lives, but fail to recognize that the new ways in which one verbally thinks about matters is “memory reconsolidation.” It is the same mechanism of change as in emotional “memory reconsolidation” of the right hemisphere. The left frontal columnar circuits are responsible for the new ways one verbally thinks. It should then be no surprise that the right cortex is also fully capable of learning new concepts and incorporating these with those that pre-existed. This involves the action columns in the right frontal lobe. Notably, if the new information involves right cortical columns with emotional associations, the so-called “reconsolidation” is perceived as a change in emotion, not a change in verbal thinking.
Similarly, with the information previously discussed in this article, I don’t believe any readers will be surprised when I say that repeating words in your head involves activity in the verbal interpreter. Let’s now take the same concept and apply it to a different action, such as watching someone using a hammer and thinking about performing that action. In that case the columns in the motor planning area located in front of the hand area of the primary motor strip and the area behind the hand area of the parietal primary somatosensory strip are activated. Just as I can repeat words in my head to fully comprehend what is said, I can repeat the physical action in my head to fully comprehend the action involved with using a hammer. This is the nature of so-called “mirror neurons” based on columnar theory.
I hope it is apparent that we learned our native spoken language in the left hemisphere. However, prior to our abilities to comprehend and speak our verbal language, we have already begun to learn our native emotional language in the right hemisphere since fewer columns are involved in the processing. If fewer columns are involved, both processing and memory formation are faster. Based on interactions with adults, the first interpersonal complex sensory memories are located in the right hemisphere. This in turn means the associated frontal columns tied to the sensory memory columns form in the right hemisphere before the action columns of the left tied to spoken language. This explains how we can have a learned receptive and expressive emotional language based on the right cortical columnar circuits which preceded and is largely independent of the left cortical verbal language.
In reference to attachment and contact comfort, being held gently but firmly while seeing the smiling face of one’s mother with the calm, soothing tone of her voice allows a complex sensory memory associated with positive feelings. With repeated similar behaviors from one’s mother and other adults then that individual will, when older, experience positive emotions with touches, smiles, and soothing voices based on reactivation of those right hemisphere memories. If as an infant one’s smiles and coos are met with similar responses from the caregiver, those expressive behaviors increase. If when crying in distress because of a wet diaper or being hungry, one’s caregiver responds promptly to remove the distress, it is learned that social interactions are important in achieving comfort and security. Such right cortical memories will later result in an individual enjoying and valuing social contact.
The opposite can happen, as therapists are aware. Being held little or roughly, with a distant, cold touch, results in an absence of positive emotions at best, and negative emotions at worst. If cries of hunger or being wet are ignored or met with a loud, harsh response, the action columns that form involve escaping and avoiding social interactions. The columns and associated memories formed first are those in closest proximity to the primary sensory and motor areas. Once formed, these basic and foundational right cortical columns are permanent, and serve as the basis for new learning which involves new higher-order columns. The result of such a difficult learning history is that the individual will, for the rest of his or her life, have problems with feeling attached and comfortable in close social interactions. Similarly, there will be problems in the expression of emotional attachment.
The foregoing descriptions involve extreme conditions, but serve to illustrate the manner in which we each form the non-detailed positive and negative sensory emotional memories of the right posterior cortex that largely determine what feels positive and negative to us in relationships. It also provides an example that we develop complex behavioral expressions (right frontal columns) that lead to relatively stable patterns (i.e. “personality”). I believe that the non-detailed emotional receptive memories determine whether giving versus taking power, control, attention, and/or things in close relationships is positive and negative. The associated action memories determine the manner in which we act in pursuit of more positive and less negative in our interpersonal interactions. Based on this, I have described what I believe to be distinct Type-T (taker) and Type-G (giver) patterns and what are the most effective ways to deal with each.
Negative emotional memories
As already mentioned, the right posterior cortical memories are the primary ones leading to maladaptive emotions. The two factors which appear to determine if the memories will be detrimental involve controllability and personal inadequacy/responsibility. If there is a high level of perceived lack of control and personal responsibility, as often happens in interpersonal relationships, there is significant impact in one’s later life. For example, having a physically and emotionally abusive parent not only impacts one’s later functioning in one’s home life, it also leads to anxiety around authority level figures, such as one’s boss. Being picked on frequently as a child/teen without fighting back often leads to adulthood anxiety with peers.
Since the influential memories are located in the right cortex, it is important to effectively engage the right cortex in developing new action columns in response to the old memories. As I have read many case descriptions using different approaches leading to desirable emotional changes/ transformations in clients, I believe there is a distinct pattern. First, there is increased anxiety when discussing emotionally charged memories. With progression, anger becomes the paramount emotion. If actively expressed in some fashion, the anger dissipates and there is a feeling of relief/resolution, often with a healthy sadness/grief. Achieving a state of forgiveness for the perpetrator appears to be the best final outcome.
I employ what is termed emotional restructuring to deal with influential past negative relationship memories. It is the only structured approach of which I am aware with specific steps to elicit the desirable emotional transformations tied to a targeted relationship within the confines of a one- to two-hour session. The first step involves the client recalling negative situations that occurred with the target individual (e.g., mother, spouse). The second step is providing the client a description of the target individual based on the Type-G or Type-T patterns previously mentioned. In relation to experiential techniques, there is a role reversal in which the client assumes the position of the target individual (and role play if needed). The experience in the role reversals allows the association of new right frontal action columns in which the client “feels” the target individual’s responsibility for the problems, accompanied by a rise in anger. The next step is the use of directed imagery for the release of anger, immediately followed by imagery to enhance self-nurturance. The directed imagery allows for the development of new frontal action columns tied to the old memories with associated perceptions of control and personal adequacy, as well as compassion for self. The fifth step involves additional information given to the left hemisphere which conveys the target individual as incapable of different behavior patterns based on his/her own learning history, with abundant examples which evoke visualization and right hemisphere involvement. The final component is a role-played forgiveness sequence in which the client acknowledges the emotional impact of the target individual’s behavior and that the individual was a victim of his/her own past. I have seen consistent success with this approach but have not had the opportunity to conduct any group research.
Conclusions
The goal of this article was to introduce the Clinical Biopsychological model as a brain-based approach to psychotherapy integration. Only limited information has been presented in specific areas, but I hope this leads to a desire for the readers to learn more. I believe the model allows clinicians to formulate case conceptualizations and treatment plans which are shared directly with clients. It provides a means to understand how various treatment techniques have their impact, so that it is feasible to refine and combine procedures in a logical manner. The theory allows for a new framework to understand interpersonal relationship behavior patterns, a structured approach in dealing with relationship negative emotional memories and a means to explain normal emotional reactions to loss. However, it also supports the importance of the therapeutic relationship and how this has positive impact. Although much of what I have described may appear to be structured and directive in nature, I do not believe this precludes a constructivist slant in therapy. If what I have discussed is accurate, the information given to clients in conjunction with improved emotional functioning and hemispheric congruence provides fertile ground for the verbal interpreter to excel in constructing meaning.
References
Alcaro, A., & Panksepp, J. (2011). The SEEKING mind: Primal neuro-affective substrates for appetitive incentive states and their pathological dynamics in addictions and depression. Neuroscience and Biobehavioral reviews, 35, 1805-1820.
Gazzaniga, M. S. (2002). Consciousness. In V. S. Ramachandran, (Ed.), Encyclopedia of the human brain (Vol. 2, pp. 31-35). New York: Academic Press.
LeDoux, J.E., and Phelps, E.A. (2010). Emotional networks in the brain. In M. Lewis, J.M. Haviland–Jones, and L.F. Barrett (Eds.), Handbook of emotions (pp.159–179). New York: Guilford Press.
Moss, R.A. (2001). Clinical biopsychology in theory and practice. Greenville, South Carolina: Center for Emotional Restructuring.
Moss, R.A. (2006). Of bits and logic: Cortical columns in learning and memory. Journal of Mind and Behavior, 27, 215–246.
Moss, R.A. (2007). Negative emotional memories in clinical treatment: Theoretical considerations. Journal of Psychotherapy Integration, 17, 209–224. doi:10.1037/1053-0479.17.2.209
Moss, R. A. (2010). Clinical Biopsychology: Could A Grand Theory Actually Exist To Allow True Psychotherapy Integration? Independent Practitioner, 30, 67-71.
Moss, R. A., (2013a). A roadmap to the cerebral cortices. The Neuropsychotherapist, 2, 114-117. doi: 10.12744/tnpt(2)114-117
Moss, R. A. (2013b). Psychotherapy and the brain: The dimensional systems model and clinical biopsychology. Journal of Mind and Behavior, 34, 63-89.
About the author
Robert A. Moss is a clinical neuropsychologist with Bon Secours St. Francis Hospital, Greenville, SC, USA. He is the Editor-in-Chief of AIMS Neuroscience. He is board certified in clinical psychology and neuropsychology. He has authored numerous professional articles and has presented at a number of professional meetings. His website is www.emotionalrestructuring.com
Important: TherapyRoute does not provide medical advice. All content is for informational purposes and cannot replace consulting a healthcare professional. If you face an emergency, please contact a local emergency service. For immediate emotional support, consider contacting a local helpline.
Find Therapists
Must Read
Creating Space for Growth: How Boundaries Strengthen Relationships
Setting healthy boundaries fosters respect, protects emotional well-being, and strengthens relationships by defining personal limits and maintaining self-care.
International Mutual Recognition Agreements for Mental Health Professionals
Mutual recognition agreements for mental health professions are rare and uneven, with major gaps in counselling, social work, and allied therapies. Read on to understand ...
Jumping to Conclusions
Jumping to conclusions is a thinking habit where we assume the worst or make judgments without enough evidence. By recognising this pattern, therapy can help you slow dow...
Case Conceptualisation
Case conceptualisation is how a therapist thoughtfully pulls together your concerns, experiences, and strengths into a clear understanding of what’s going on. This shared...
Guided Discovery
Guided discovery invites clients to arrive at their own insights through collaborative questioning and reflection. Instead of being told what to think, individuals learn ...
About The Author

New Therapist Magazine
Pietermaritzburg, South Africa
“An independent, subscription-based magazine for mental health therapists, produced by journalists and therapists on five continents.”
New Therapist Magazine is based in Clarendon, Pietermaritzburg, South Africa.


