
Good Grief

❝A contemporary orientation to bereavement counseling❞
How do complications in grieving present themselves in the course of therapy with the bereaved, and how can practicing therapists respond to them? In this article one prominent grief therapist, theorist and researcher reflects on the emerging diagnosis of complicated grief in light of more adaptive trajectories through loss, and outlines the relational and technical features of demonstrably effective clinical interventions. Viewed constructively, loss challenges the taken-for-granted assumptions of life, and can prompt significant, and often salutary revisions in our life stories. Drawing on contemporary models and methods, counselors and psychotherapists can make a contribution to this outcome.
The field of grief therapy is in ferment. Increasingly, time-honored assumptions regarding grieving as a relatively predictable series of emotional stages that proceed largely on an intrapsychic stage and that eventuate in the breaking of bonds to the deceased are coming under review, and often revision or replacement. In their place, new, empirically informed models have gained currency, which view grieving as a multidimensional process of meaning making that unfolds not only within people but also between them, with adaptive outcomes embracing the reconstruction of attachment to the deceased rather than its relinquishment. In this interview, prominent bereavement theorist and therapist Robert A. Neimeyer answers questions about the upshot of these developments for therapists who encounter clients in the wake of life-altering loss. His humanistic belief in the reality of resilience notwithstanding, Neimeyer acknowledges the unique complications that can accompany the death of a loved one, and sketches the role of therapeutic presence, process and procedure in addressing the variegated needs brought to clinicians’ offices in the wake of tragic bereavement.
Healing from trauma is possible with the right therapist. TherapyRoute lists trauma-informed professionals ready to support you.
Find a Trauma Therapist
John Soderlund: Bob, the work of Dr. George Bonnano suggests that the majority of people who experience a significant loss react with a surprising degree of resilience, to the extent that the grief process can, in the longer term, be a positive experience for them. This tends to counter a prevailing, if rather archaic, view that counseling is routinely a valuable process to help people deal with bereavement. With this in mind, can you reflect on what variables therapists ought to bear in mind when first encountering somebody who has been referred to them on account of a recent bereavement?
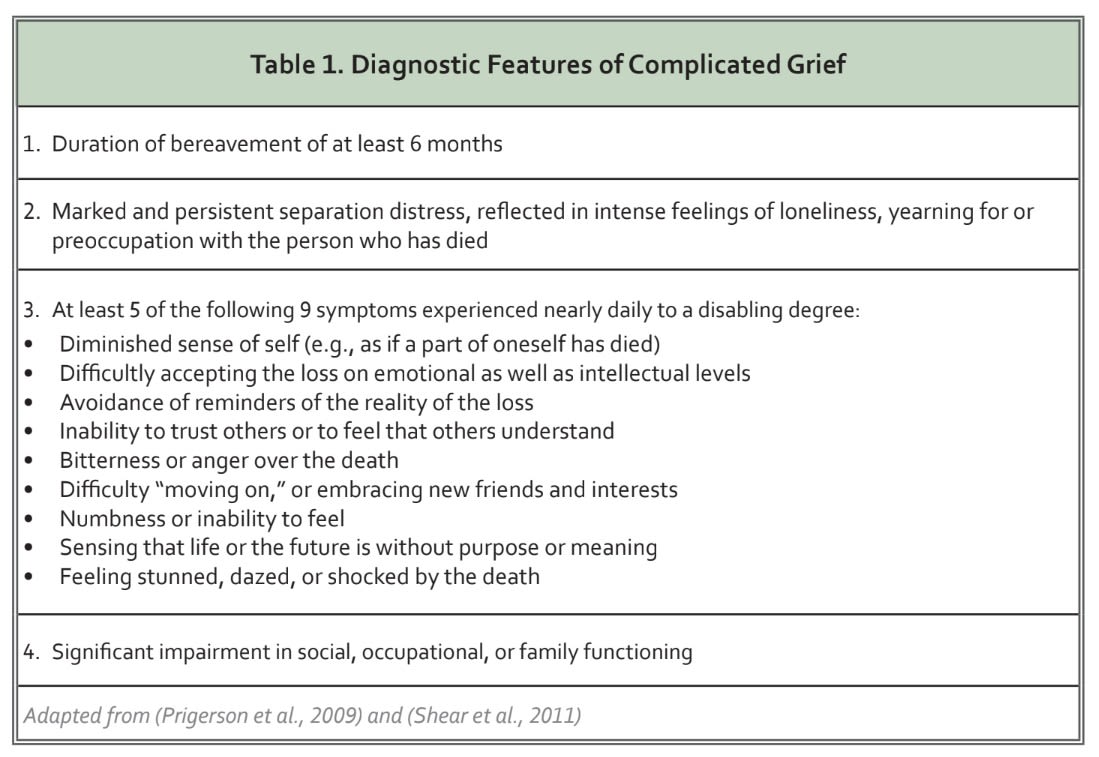
Bob Neimeyer: Well, to say that the death of one’s child, partner, sibling, parent or friend could in the long run be considered a “positive experience” may be a bit of an overstatement; I’ve met very few grieving people who wouldn’t give back in a heartbeat any degree of personal growth they’ve achieved to have their loved one back physically in their lives. But at the same time, resilience is a clear reality for close to half of the bereaved, who manage to weather the storm of mourning surprisingly quickly, finding their footing in the world once again within a matter of a few months, even if they continue to miss their loved ones keenly. For many others, the loss more profoundly disrupts their mood and functioning for several months, but they too ultimately grieve adaptively, integrate the loss into their lives, and return to their emotional baseline while revising their life routines and goals accordingly. Another 25%, however, tend to fare worse, experiencing exacerbations of previously problematic patterns (e.g., of chronic depression or substance abuse), family- and work-related conflicts, or—of special interest in the present context—a condition known as complicated grief or prolonged grief disorder, experienced by about 10% of the bereaved. To give your readers a quick orientation to this significant clinical problem, I’ll include a “clinician’s toolbox” to help them identify its key diagnostic features (see Table 1). We can explore this condition a little more thoroughly with a focus on its assessment and treatment later in this interview. I guess the point I’d like to make at the outset is that grieving can lead to surprisingly different outcomes, only a minority of which are likely to benefit from psychotherapy. Of course, that minority is enough to keep us busy for the rest of our professional lives!
Before shifting to more discussion of complicated grief trajectories, however, I’d like to loop back to your earlier implication about the upside of grief. Beyond resilience per se, which refers essentially to a rapid return to baseline following a significant stressful event, a surprising number of people also report substantial post-traumatic growth (PTG) in the long-term wake of loss. As defined by Calhoun and Tedeschi, PTG refers to a cluster of developments in the wake of a “seismic” life transition, which include a greater sense of strength and maturity, deepening of relationships and compassion for the suffering of others, keener appreciation for life, greater readiness to embrace possibilities, and often a renewal of spiritual and philosophical frameworks for living. Nothing about this is inevitable, of course, and our own research and that of others suggests that PTG is typically a hard-won outcome of a good deal of painful reflection and meaning-making, which is probably most accessible when the distress of bereavement is sufficiently intense to challenge life as usual, but not so overwhelming as to make constructive change impossible. Figure 1 depicts the sort of curvilinear relationship between the intensity of grief and the degree of personal growth that we’ve observed in our research.
John: Some of what you were saying about the different trajectories of bereavement reminds me that many medically inclined mental health professionals tend to roll grief into their list of pathological processes if the attendant emotions persist beyond a "reasonable" period. If the latest edition of DSM is anything to go by, what is considered a reasonable period of grieving is being steadily reduced. What, in your opinion, should be considered pathological in the grieving process and what should be considered normal variations in the process of grieving?
Bob: Well, truth be told, the DSM 5 probably isn’t the best source to go by! What I mean by that is that it seems to me to fail in at least three ways. First, many people, including major advocacy groups for the bereaved themselves, argue that it risks pathologizing normal grief as “major depression,” diagnosable by its criteria within two weeks following the loss. Whether or not this is scientifically legitimate on the basis of the consistency of depressive symptomatology following the loss of a loved one or another major stressor, it is likely to open the door to widespread prescription of antidepressants to mourners, even if specialized forms of psychotherapy have a stronger track record of efficacy when grief is, in fact, complicated. Second, it fails to recognize that grief as a form of separation distress has more in common phenomenologically and even neurologically with anxiety than with depression as such, and therefore often calls for different treatment. And finally, even though the DSM-5 includes “Persistent Complex Bereavement Disorder”— apparently an awkward attempt to combine the commonly used terms “complicated grief” and “prolonged grief disorder” into a single mouth-filling moniker—it classes it as a “condition for further study,” even though the evidence base for it is considerably stronger than that for many of the conditions included in the manual. Moreover, it defines the condition with a hodge-podge of paraphrased and conjectural diagnostic features, rather than the scientifically established criteria summarized in Table 1. Thus, at minimum, the DSM-5 missed the opportunity to recognize what was uniquely difficult about complicated grief, while blurring its distinction from garden-variety depression.
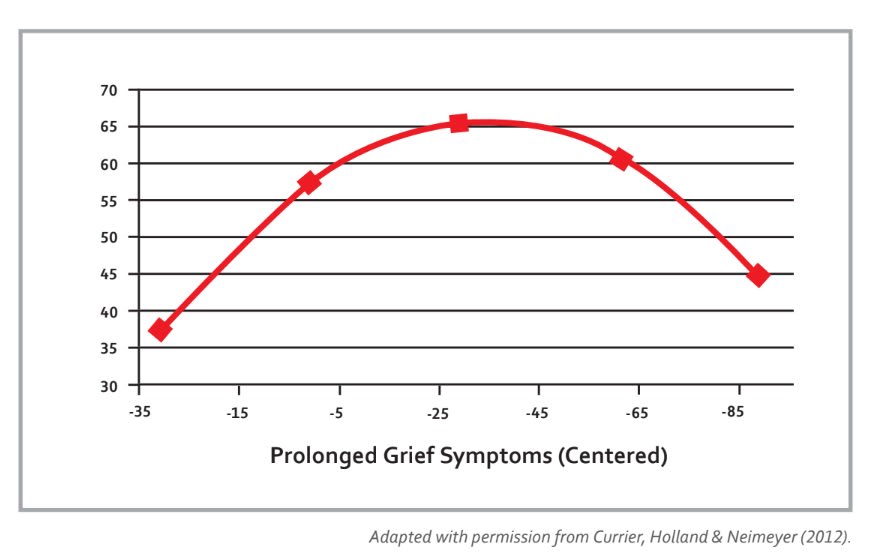
Figure 1. The nonlinear association between prolonged or complicated grief and posttraumatic growth.
Far more useful, in my view, is the approach to diagnosis of prolonged grief disorder (PGD) that appears to be moving forward in the current revision of the World Health Organization’s International Classification of Disease (ICD-11), which classes PGD with other “stress related disorders,” identified by symptoms that conform closely to those listed in Table 1. This means that common experiences of crying, missing a loved one, and so on in the aftermath of adeath are regarded as normal and expectable reactions, whereas others like pervasive separation distress, profound disconnection from others, and sensing that the future is bleached of purpose a year or more after the loss, in the context of marked deterioration in the client’s social or occupational functioning, would be a cause for clinical concern. Alongside other possibly comorbid conditions such as depression, generalized anxiety or post-traumatic reactions (especially in the aftermath of sudden, violent or untimely death), this could call for clinical intervention.
John: Okay. So what should a practicing therapist know about intervention when grief is complicated or prolonged? For example, much is made of the practice of "presence" in grief counseling. Can you unpack what this means and why its so crucial to this kind of counseling?
Bob: Certainly. When I think about grief therapy, or any responsive psychotherapy for that matter, I think in terms of three dimensions: presence, process and procedure. By presence, I mean the capacity to offer full availability and attention to the client’s concerns, undistracted by our own agendas. It is more about being than doing, allowing ourselves to “indwell” our clients’ narratives of loss, to feel ourselves into their stories, to be moved by their love for the deceased and touched by their brokenness. At the same time, this authentic and unflinching willingness to stand in the pain rather than merely rush to mitigate it provides a safe “container” for the client’s own exploration of his experience, ameliorating the sense of being alone in a silent story of nameless anguish. In this intersubjective field of vivid presence, characterized by the time-honored practice of client-centered listening and reflection, we in a sense take up residence in our clients’ meaning systems, understanding experientially the deep wellsprings of their grief, alongside their resources for living with and learning from it. Like Martin Buber’s concept of the I-Thou relationship, it is a fundamentally respectful stance that accords full humanity to our clients, prior to any preoccupation with their diagnosis or case conceptualization.
Within this relational frame, therapists then attend like delicately attuned instruments to the process of therapy, that speaking-turn-by-speaking-turn interaction in which we read between the lines of what clients tell themselves about the loss to discern the conjunction of their current need and readiness that identifies specific points of intervention. For me, grounding in process implies a lively alertness to our clients’ subtle and obvious displays of emotion—a slight break in speech, a welling up of sudden tears, a slowing down into reflective processing of an emerging awareness. By extension, it implies equal attention to verbal, co-verbal and nonverbal channels of communication, not only to what is said and how it is said, but also to the bodily movements or facial expressions that accompany it. #is leads naturally to a “bottom-up” approach to therapy that is more experiential than psychoeducational, in a sense leading a client from one step behind toward clearer encounters with his or her emotions, relationships and possibilities, rather than directing therapy in a “top down” manner to speak the language of the therapist’s preferred theory, and be trained in our preferred techniques. But more broadly, responsiveness to process is essential even to more directive therapeutic approaches or strategies, as it tells us when a client is specifically primed to process the event story of a suicide or accidental death, for example, or when they are needing to revisit the previously unexpressed problems or unrealized potential in the relationship to the deceased. In this sense, presence and process provide a container for not only the client’s exploration of emotional meanings of the loss, but also for the therapist’s utilization of specific procedures.
John: What are some of those procedures? And have any of them actually been researched in the sense of having an evidence base that supports their use with clients suffering from complicated grief?
Bob: Well, the answer to that question would be a book in itself, and indeed I can recommend a few of them! (See Recommended Readings below.) Basically, as a constructivist therapist, I view clients in acute grief as struggling with two key narrative processes in their attempts to make meaning of the experience. On the one hand, clients often feel the need to process the “event story” of the loss itself, to in some way wrap their hearts and minds around what has happened, what it means, and what it portends for their lives going forward. On the other hand, they frequently need to access the “back story” of their relationship with the deceased, not only to sort out their “unfinished business” of conflicts or regrets in the relationship, but also to reconstruct their attachment bond with their loved one into a form that is sustainable now. In other words, clients need to make sense—viscerally in their bodies, experientially in their emotions, conversationally in their families, and spiritually in terms of their abiding life philosophies—of a profound rupture in their life stories, as well as to re-write the terms of their attachment to the deceased. It’s a tall order for many, particularly when the death was traumatic, intentional, sudden or untimely, and when the relationship was complicated or eclipsed by the narrative of a violent death or a grimly progressive illness that threatens to overshadow the living image of the person we knew and loved.
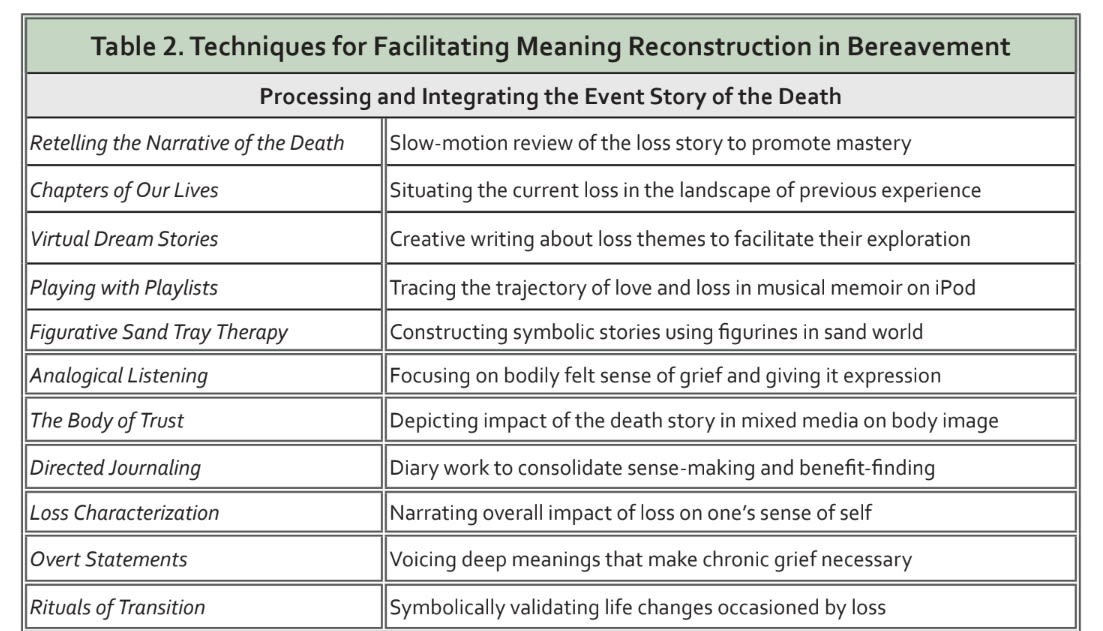
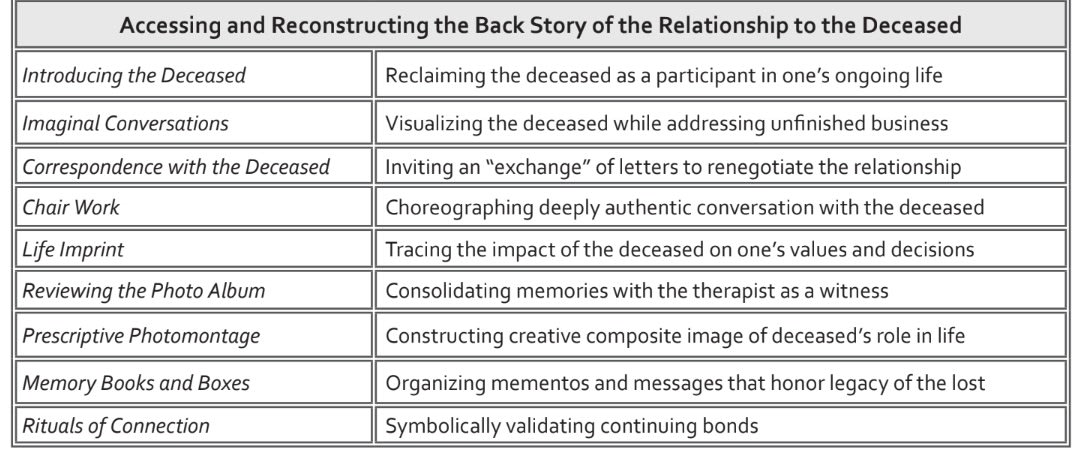
Viewed in these terms, grief therapy often entails an interplay between two different kinds of interventions, one centered on the event story of the death and its larger implications for the client’s life, and the other focused on the lost relationship (see Table 2). I allow myself to be led by the client to what he or she most needs and stands ready to address, as explicitly requested or more commonly implicitly revealed by his or her presentation. For example, I may begin by inviting a widow to tell me how I can be useful to her, which tends to lead to an abbreviated account of the loss and her subsequent yearning for her husband or her sense of feeling lost without him. Alerted to the significance of the interrupted relationship, I might then invite the client to introduce me to the deceased, by sharing more about the character of their relationship or their family experience. This might naturally lead to evocative correspondence with the deceased or chair work to affirm their continuing bond or to address unfinished business in the relationship, or simply to memorializing the loved one in a photo album or meaningful ritual that preserves a sense of continuity and connection between the living and dead. All of these interventions and many others bear on the back story of the relationship, opening it to fresh readings in the present.
At other times, however, the client clearly needs to revisit the story of the illness or death itself, particularly when it was violent, unanticipated, and involved complicated human intention (as in suicide or homicide) or inattention (as in a fatal accident or medical malpractice). In such cases I join my client in restorative retelling, essentially a prolonged, fearless recounting of the circumstances of the death in slow-motion detail, giving voice to the horror of what the client witnessed or imagined, while helping him or her contain it, breathe through it, master it and modulate the associated emotions. Like the prolonged exposure therapies to which it is akin, this form of deliberative processing can help a client integrate a difficult experience, imagine the more empowered stance that he or she would have taken in comforting the loved one at the time of dying if this had been possible, and take steps to place the loss into the ongoing sequence of chapters of their lives, rather than view it as the end of the story. Alternatively, we can encourage our clients to engage in directed journaling, prompted by questions about the sense made of the loss or the unsought benefits or learning that might be found in it, or to make use of any of a number of metaphoric or creative practices to help them express and explore their grief to give it voice and validation. All of these procedures and a hundred others are described clearly and succinctly in the recommended readings, and illustrated with actual case studies of their use.
Finally, in response to your question about the evidence base for such practices, I am pleased to say that a growing literature is documenting the specific efficacy of retelling, exposure, imaginal conversations, directed journaling, expressive arts and other interventions in addressing the unique challenges of complicated grief. There is more to learn, of course, but the documentation of a wide range of creative procedures holds promise that we can offer something of relevance to a diverse community of clients grieving a wide variety of losses.
John: All right, let me finish with a big question suitable for this big topic. Various psychoanalytic writers, from Freud onwards, have paid considerable attention to how we think about, relate to and make sense of our mortality. !is interest in death and how we negotiate the finite nature of our existence appears to have been driven from the prominent position it has held historically in many philosophical traditions. Do you think that we as a species are increasingly avoiding the issue? Do we have a pathological inclination to deny our own mortality and that of our most important others? If so, what are the implications of this?
Bob: Pathology, I suppose, is in the eye of the beholder. Is it more pathological for humans, like the other sentient beings who share our small planet, to orient our limited conscious resources toward engaging and problem solving the events of our lives, or toward anticipating the eventuality of our deaths? Freud famously argued that “the unconscious cannot conceive of its own death,” but it is clear that as partially conscious creatures, we can indeed do so, if only with some degree of effort and normative anxiety. Existentialists would go so far as to say that we only live authentically to the extent that we courageously contemplate our ultimate nonbeing, and then return from peering into this “abyss” with a clarified will to live fully in the light of our highest values. Because we are soft bodies in a hard world, we also can appreciate more keenly our collective vulnerability to illness, injury and extinction, and live more prudently and compassionately as a result.
Finally, with respect to bereavement, we are forced to acknowledge another existential truth: we are wired for attachment in a world of impermanence. Even if more narrowly “medical” approaches to therapy ignore the fact, ultimately, every person, every place, every project and every possession to which we are attached we will one day lose, at least in an earthly sense. And so learning how to live with this looming reality, learning literally from loss, shapes who we become as individuals, families, communities and cultures... just as it can shape how we practice psychotherapy.
Recommended Readings
Currier, J. M., Holland, J. M. & Neimeyer, R. A. (2012). Prolonged grief symptoms and growth in the first two years of bereavement: Evidence for a non-linear association, Traumatology, 18, 65-71. [Study of posttraumatic growth as a function of level of grief experienced.]
Currier, J. M., Neimeyer, R. A. & Berman, J. S. (2008). The effectiveness of psychotherapeutic interventions for the bereaved: A comprehensive quantitative review. Psychological Bulletin, 134, 648-661. [Systematic review of outcome literature on grief therapy.]
Galatzer-Levy, & Bonanno, G. A. (2012). Beyond normality in the study of bereavement: Heterogeneity in depression outcomes following loss in older adults. Social Science & Medicine, 74, 1987-1994. 10.1016/j.socscimed.2012.02.022 [Analysis of different trajectories of grieving and their frequency.]
Neimeyer, R. A. (Ed.) (2012). Techniques in grief therapy: Creative practices for counseling the bereaved. New York: Routledge. [Handbook of 96 methods of grief therapy, with instructions for each and a case study illustrating its application.]
Neimeyer, R. A. (2009). Constructivist psychotherapy. New York and London: Routledge. [Practical and readable presentation of meaning-oriented approach to psychotherapy with numerous discussions of strategies and case studies focused on bereavement.]
Neimeyer, R. A., Harris, D., Winokeur, H. & Thornton, G. (Eds.) (2011). Grief and bereavement in contemporary society: Bridging research and practice. New York: Routledge. [Comprehensive handbook on new conceptualizations of grief, with focus on different types of loss, special populations and therapeutic issues and methods; each chapter is coauthored by prominent researchers and practitioners to thoroughly integrate scholarship and practice.]
Prigerson, H. G., Horowitz, M. J., Jacobs, S. C., Parkes, C. M., Aslan, M., Goodkin, K., Raphael, B., Maciejewski, P. K. (2009). Prolonged grief disorder: Psychometric validation of criteria proposed for DSM-V and ICD-11. PLoS Medicine, 6(8), 1-12. [Review of the development of criteria for complicated grief/PGD and a field trial demonstrating their validity.]
Shear, M. K., Simon, N., Wall, M., Zisook, S., Neimeyer, R., & al., et. (2011). Complicated grief and related bereavement issues for DSM-5. Depression and Anxiety, 28(2), 103-117. doi: 10.1002/ da.20780 [Review of conceptualization of complicated grief and implications for treatment, with emphasis on an attachment theory framework.]
Thompson, B. E. & Neimeyer, R. A. (Eds.) (2014). Grief and the expressive arts: Practices for creating meaning. New York: Routledge. [Comprehensive handbook detailing dozens of grief therapy techniques using visual arts, music therapy, dance and movement, creative writing and theatre and performance, giving explicit instructions and case examples to illustrate each.]
About the interviewee
Robert Neimeyer is Professor in the Department of Psychology, University of Memphis, where he also maintains an active clinical practice. Since completing his doctoral training at the University of Nebraska in 1982, he has published 27 books, including Techniques of Grief Therapy: Creative Practices for Counseling the Bereaved and Grief and Bereavement in Contemporary Society: Bridging Research and Practice (both with Routledge), and serves as Editor of the journal Death Studies. The author of over 400 articles and book chapters, he is currently working to advance a more adequate theory of grieving as a meaning-making process, both in his published work and through his frequent professional workshops for national and international audiences. Neimeyer served as President of the Association for Death Education and Counseling (ADEC), and Chair of the International Work Group for Death, Dying, & Bereavement. In recognition of his scholarly contributions, he has been granted the Eminent Faculty Award by the University of Memphis, made a Fellow of the Clinical Psychology Division of the American Psychological Association, and been recognized as an Honored Associate of the Viktor Frankl Association, as well as a recipient of the Phoenix Award: Rising to the Service of Humanity by the MISS Foundation.
Important: TherapyRoute does not provide medical advice. All content is for informational purposes and cannot replace consulting a healthcare professional. If you face an emergency, please contact a local emergency service. For immediate emotional support, consider contacting a local helpline.
Find Therapists
Must Read
Creating Space for Growth: How Boundaries Strengthen Relationships
Setting healthy boundaries fosters respect, protects emotional well-being, and strengthens relationships by defining personal limits and maintaining self-care.
International Mutual Recognition Agreements for Mental Health Professionals
Mutual recognition agreements for mental health professions are rare and uneven, with major gaps in counselling, social work, and allied therapies. Read on to understand ...
Jumping to Conclusions
Jumping to conclusions is a thinking habit where we assume the worst or make judgments without enough evidence. By recognising this pattern, therapy can help you slow dow...
Case Conceptualisation
Case conceptualisation is how a therapist thoughtfully pulls together your concerns, experiences, and strengths into a clear understanding of what’s going on. This shared...
Guided Discovery
Guided discovery invites clients to arrive at their own insights through collaborative questioning and reflection. Instead of being told what to think, individuals learn ...
About The Author

New Therapist Magazine
Pietermaritzburg, South Africa
“An independent, subscription-based magazine for mental health therapists, produced by journalists and therapists on five continents.”
New Therapist Magazine is based in Clarendon, Pietermaritzburg, South Africa.



