
Dynamics Anonymous, by Philip J. Flores

❝An attachment theory and relational models perspective of the psychodynamics of Alcoholics Anonymous❞
In a number of comprehensive and extensive literature reviews on addiction treatment, the twelve- step abstinence model or the AA disease concept approach was identified as the most widely used form of addiction treatment in the USA (Miller, 1995, McKeller, J., Stewart, E. & Humphreys, K (2009). This fact was juxtaposed with another surprising discovery that, despite the widespread popularity of this treatment approach, the twelve-step abstinence model has been largely and arbitrarily excluded from many previous reviews on addiction treatment. Despite the extensive utilization and immense popularity of the twelve-step, abstinence-based approach for addiction treatment, this model remains ignored and maligned by many researchers and clinicians. This remains even though there have been a number of respected outcome studies supporting AA effectiveness and the evidence is clear that AA fits the criteria for Evidence Base Practice. (McKeller, J., Stewart, E. & Humphreys, 2009. Project MATCH, 1997)
Sometimes you just need someone qualified to talk to. Find a counsellor near you — independent, professional, and ready to listen.
Find a CounsellorMisconceptions About Alcoholics Anonymous
For decades, the relationship between clinicians, or researchers, and self-help groups such as AA was predominantly one of mutual disregard and distrust, with the possibility of constructive interaction receiving scant consideration. At least part of this polarization stemmed from the fact that members of AA, before finding acceptance, help, and constructive change as a result of their involvement in the AA program, had unsuccessfully sought help from psychotherapists. Many psychotherapists, on the other hand, have found trying do therapy with addicts or alcoholics along traditional lines both frustrating and unrewarding. Both groups were equally dissatisfied in their interactions with each other. AA members viewed professional treatment providers as incompetent, uncaring, and distant. At the same time, many clinicians saw alcoholics and addicts as unmotivated, manipulative, and untreatable.
However, within the last couple decades, various developments have brought many professionals and the AA program closer together. It has been a common assumption that peer or mutual-help groups have always had grassroots rather than professional origins. However, as Lieberman and Borman (1979) have noted, there has, in fact, been appreciable professional input in the formation and encouragement of several self-help groups. This is the case with AA, as can be seen if one examines the historical roots of the twelve-step program. AA’s chief architect and author of the Big Book, Bill Wilson (1939), had read William James’s classic text, The Varieties of Religious Experience (1902), extensively, and James’s philosophical position of pragmatism is a theme that runs throughout Alcoholics Anonymous’ program of recovery. Wilson also had extensive correspondence with Carl Jung, and Jung’s influence is strongly reflected in the spiritual emphasis of the program. Add Ralph Waldo Emerson’s influence from the Oxford Group Movement with its ties to Immanuel Kant and the Transcendentalists and it becomes apparent that there is a solid theoretical foundation to the AA program. Kurtz (1982) also notes that there are “profound parallels that exist between the AA insight and the animus of existential philosophy” (pp. 38-39). AA’s philosophical and theoretical roots are diverse and they run deeply. All of this suggests, as Kurtz later write, that it is time to take the intellectual influence of AA seriously. This is a recommendation that absolutely applies to psychodynamically oriented theorists and practioners.
The relational models: An integration & alternative perspective on AA
It is important to have a comprehensive meta-theory of addiction that not only integrates diverse mental health models with the disease-concept, but also furnishes guidelines for clinical practice that are compatible with existing treatment strategies. Any proposed theory—no matter how comprehensive and intellectually satisfying it is—will not maintain credibility if its basic premises fly in the face of applied practical experience and the fundamental realities of successful clinical applications. Since most addiction specialists who deliver treatment adhere to an abstinence-based treatment approach that is closely aligned with 12-step treatment philosophy, any theory is doomed to be ignored if it contradicts direct clinical experience of those who work with this population on a consistent, daily basis.
Attachment theory accomplishes this aim. With its rich heritage and solid grounding in psychodynamic theory, it provides a respected theoretical perspective that helps legitimize the recommendations of the abstinence-based treatment approach. Most importantly, none of attachment theory’s basic premises conflict with any of the principles of the AA program. Lewis, et al (2000) support this position when they write, “An addict’s bulwark against relapse involves more communion that cognition, as Alcoholics Anonymous and its multiple variants demonstrate. Gathering like people together to share their stories imbues a wordless strength, what Robert Frost called in another context ‘a clarification of life—not necessarily a great clarification, such as sects and cults are founded on, but a momentary stay against confusion.’ The limbic regulation in a group can restore balance to its members, allowing them to feel centered and whole.”
An attempt to synthesize and integrate the seemingly divergent perspectives of AA and attachment theory can lead to a more thorough understanding and appreciation of the therapeutic stance that must be taken when treating addiction. Such an investigation can also supply a firmer theoretical foundation for those dissatisfied with AA because of its perceived lack of rigorous scientific underpinnings. The integration of these diverse approaches can also furnish a more expansive view of AA, alleviating some of the misgivings that critics have of the program. Hopefully, this will not only provide needed clarification and elaboration, but will help establish a more harmonious relationship among these conflicting perspectives.
Accepting attachment theory as a credible alternative explanation for the etiology and treatment of addiction also permits the recognition of additional contributions from other related perspectives. Psychodynamic theory has gone through an exciting evolution in the last half of the twentieth century. In contrast to a “one person” psychology (i.e. a neutral therapist tries to understand the unconscious determinants of the patient’s aberrant behavior), the relational models are a “two person” psychology. From this perspective the patient’s psychology is inextricably connected to context, which is to the psychology of the therapist or person with whom the person is interacting. While the understanding that is developed in the psychotherapeutic context is related to the patient’s personal history, it remains the case that the behavior demonstrated is always a function of the current situation and psychological states of every participant in the relationship. Relationships, therapeutic and social, are shaped by projections, assumptions, hopes, wishes and fears of all participants. The development of the relational models has shifted the focus away from intra-psychic struggles to an exploration of the interpersonal or relational difficulties that contribute to a person’s present situation. Most importantly, the relational perspective has ushered in more innovative ways for understanding addiction.
Self psychology (1977) was the first theory to offer a comprehensive theoretical description that bridged the gap between the abstinence-based treatment specialists and the psychodynamic-oriented psychotherapists. Kohut’s formulations were influenced by, and an extension of, the earlier work of the relational models that were developed by Bowlby (1973) and others (i.e. Guntrip, 1974; Fairbairn, 1952, Winicott, 1965) at the Tavistock Clinic in London. The object-relations school helped shift psychoanalytic thinking from classical drive or instinct theory to a relational approach with its greater emphasis on adaptation, developmental arrestment, and deficits in self-structure.
Attachment theory, like self psychology, can be considered an offspring of object relations theory. While these three theories share important similarities, they hold different allegiances to classical drive theory. The most decisive factor that differentiates attachment theory from the other two theories is the degree to which it differs from classical drive theory on the importance of attachment. Attachment theory holds firmly to the position that the pains, joys, and meaning of attachment cannot be reduced to a secondary drive. Attachment is recognized as a primary motivational force with its own dynamics (Bowlby, 1980).
Bowlby recognized that natural selection favors mechanisms that promoted parent-offspring proximity in an environment of evolutionary adaptation. Attachment is not just psychologically driven, but is propelled by powerful biological needs for interpersonal closeness. A primary biological function is to secure assistance and survival in the case of adversity.
Bowlby (1979) and Kohut (1975) are the first credible theories that provided a practical alternative rationale for the addiction cycle that is not only compatible with the disease concept, but expands it by providing a more complete and intellectually satisfying theoretical explanation as to why AA works as it does. Both attachment theory and self psychology not only help broaden the theoretical implications for treatment, they are in complete harmony with AA and complement the way 12-Step programs treat chemical dependency. Kohut and Bowlby’s perspectives also provide inherently valid alternative explanation for why 12 Step programs work as they do and how the curative forces in these programs have a direct relation to the strategies that need to be emphasized when treating patients suffering from substance abuse disorders.
Addiction, from an attachment theory perspective, holds one basic and simple premise about treatment: Until substance abusers are able to develop the capacity to establish mutually satisfying relationships, they will forever remain vulnerable to relapse and addiction. To successfully treat addiction, the addicted individual must learn how to establish healthy relationships. While this overly simplistic portrayal of attachment theory gets to the heart of the matter, it does not do justice to the intricate complexity of accomplishing such a modest maneuver. To keep the significance of attachment theory’s primary premise in perspective, it is important to remember that attachment theory holds the position that substance abuse is both a solution and a consequence of a person’s impaired ability in developing healthy attachments. Consequently, if the addict or alcoholic is to achieve abstinence and sobriety, he or she must first detach from their primary destructive relationship to substances and then develop the capacity for healthy interpersonal attachment.
Self Psychology
Heinz Kohut’s (1972) work with patients whose central disturbance involved feelings of emptiness and depression is in many important ways an extension of Bowlby's observations concerning the difficulties that occur when a child’s developmental need for secure attachment is disrupted. Kohut extended psychoanalytic thinking beyond its standard concept of drive theory so that narcissistic vulnerabilities could be better understood as a consequence of the patient's inadequately formed or damaged sense of self. Like Bowlby, Kohut emphasizes the critical importance of parental responsiveness in the development of internal mental structures for self-control and the eventual emergence of individuality and the capacity for mutuality. Kohut stressed that a child's nuclear-self is formed during infancy and embodies the fundamental self-esteem, ideals, and ambitions of the child. The nuclear self is bipolar, organized around two anchor points of ideals and ambitions. In his final book (1984), Kohut added a third constituent of the self, which involves the maturation of the alter ego or twinship needs.
Attachment with a primary caregiver allows the various agencies, drives, and conflicts of the mental apparatus to become unified into an integrated sense of self. Kohut defined the self as “a unit, cohesive in space and enduring in time which is the center of initiation and a recipient of impressions” (Kohut, 1977, p. 99). However, the formation of the nuclear-self does not take place in relation to overt praise and rebuke. Rather, it is the empathic, nonverbal, intuitive responsiveness of the mother to her child's needs, which validates healthy striving for autonomy and identity. The atmosphere the parent creates either integrates or fragments the nuclear-self. It is not so much what the parents do, as much as whom they are that determines developmental outcome.
Empathy
From the perspective of self psychology, a child needs empathic attunement from parental figures in order to develop a cohesive self. A cohesive or “bipolar self is a developmental achievement of transforming the archaic grandiose self in self-assertive ambitions and the idealized self into mature values and ideals” (Stone, 1992, p. 335). Minor or sporadic empathic failures are not deleterious. In fact, periodic lapses facilitate the crucial process of transmuting internalization. Optimal frustration within the context of a “holding environment” provided by a “good enough mother” actually facilitates the building of psychic structure and the internalization of functions previously provided by external objects. Since Kohut attributed the lack of empathy and attunement as a primary contributor to psychopathology, he reasoned that the use of empathy as a therapeutic tool was crucial in the restoration of the self. Empathy or “vicarious introspection” becomes the primary mode of data gathering for self psychologists. The therapist’s task is to identify the self-object functions that the patient requires, which are activated and demonstrated in the transferential relationship. Since it was the parent’s original failure to adequately serve this function that initiated the child’s misdirected search for regulation through dysfunctional channels (i.e. alcohol, drugs, sex, etc.), one key element in the repair of the developmental arrestment can be provided if the therapist makes him or herself available as a self-object.
Narcissism
One of Kohut's primary contributions to psychoanalytic theory is a change in the way narcissism is conceptualized. Kohut legitimated narcissism as a normal developmental process necessary for a healthy, age-appropriate need for object relatedness and attachment.
Self-object
Another person “is a self-object when it is experienced intrapsychically as producing functions that evoke, maintain, or positively affect the sense of self” (Wolf, 1985, p.271). A self-object is neither a self nor an object; rather it is a subjective aspect of a function performed by a relationship. Self-object transferences, like substance use, are attempts to complete a process initiated, but uncompleted from childhood. Kohut believed that we never give up the hope for completing ourselves. In a similar fashion, Paul Ornstien (1982), speaking to the importance of maintaining the therapeutic frame and the therapeutic alliance added, “The self is always searching for the right environment to complete itself.”
Kohut made the important distinction between healthy and pathological narcissism. Phase-appropriate, empathic responsiveness to the child's self-object needs is essential for the cohesion and development of the self and leads to healthy self-esteem. Without the idealizing or mirroring self-objects, a child is likely to grow up with narcissistic vulnerabilities leading to disturbance and difficulty with affect regulation, increasing the potential for addictive behavior. Consequently, the vulnerable individual is left without the internal structure necessary to manage the emotional injuries and disappointments (affect dis-regulation) that are sure to follow later in that life. As Bacal (1985) writes, “. . . the defects in the self produced by faulty responses of self-objects lead this individual to establish what Kohut called transference-like states, where he looks for self objects in his later life to provide him with the responses which he missed in order to repair the self.” (p. 488)
From this perspective, Bacal is suggesting that transferential relationships are essentially attempts at self-repair. Bacal’s position is similar to the self-medication hypothesis of Khantzian (1982). Both Khantzian and Kohut postulated that the use of substances and archaic self object relationships share a similar function: each is a compensatory driven behavior reflecting desperate and futile attempts to shore up the defective self. Evidence gathered by Kohut and others (i.e. Wolf, 1988; Stolorow & Atwood, 1987) over the years in their work with patients suffering from narcissistic vulnerabilities have led to the identification of seven common self-object tranferences, outlined below.
Self-object Relationships & Transferences
1. Mirroring:
A response that confirms the child’s innate sense of vigor, importance, and uniqueness. It is the “gleam in the mother’s eye” as she is empathically attuned with the child’s feelings and interests. From this experience, the child develops healthy narcissism and grandiosity.
2. Idealizing:
If the child is presented with a strong, soothing self-object who allows and provides idealization, the capacity for healthy ideals, values, and principles is internalized.
3. Alterego or Twinship:
A firm sense of self, resulting from the optimal interactions between the child and self-objects make up this third constituent in relation to the first pole (mirroring) from which emanates the basic strivings for power and success, and the second pole (idealization) that harbors the basic ideal goals and values. The core of the personality is determined by the tension arc in the intermediate area of basic talents and skills, which is established between ambitions and ideals. The need to belong to something greater than oneself, to be a human among humans, is the antithesis of alienation and isolation.
4. Adversarial:
The need to compete and exert one’s full potential without fear of destroying the other person. For a child, it’s the need to be able to play aggressively without fear of destructive retaliation. For an adult, it is the confidence that the other person will tolerate your anger and work through disagreements without the relationship being destroyed.
5. Efficacy:
The experience of having importance and significance in relation to another person. The feeling that my presence, responses, and actions can have a positive impact on another person; that I can be of help and of importance to someone.
6. Self-delineating:
A relationship with an object that promotes individuation and the separation of the self without the threat of loss of attachment.
7. Witnessing:
The need for a self-object to be a witness and provide emotional understanding for the injustices or wrongs that were inflicted on the individual.
AA & Self-Object Functions:
Self psychology’s concepts of mirroring, idealization, and a transformational or corrective twinship provide alternative ways to explain how AA is helpful to its long-term members. Mirroring takes place when the member feels they are seen for who they truly are and when they have a positive influence on others. Those suffering from deficits in this area (mirror-hungry personalities) will often get their previously unmet needs for healthy grandiosity, exhibitionism, and respect gratified by the attention that their continual sobriety brings. Idealization, whether of a sponsor, the group, or of one’s Higher Power, is in evidence when members tell of feeling bolstered by identification with some greater source of strength and wisdom. Members with longer periods of abstinence and sobriety serve as important role models that spur others on to emulate. Twinship is operating when members speak of the healing effect of belonging to the group and finding peers with similar experiences. Many of the other self-object functions are provided through continual twelve-step work (helping others) and sponsorship.
Clinical Example
After his parents had died, Cecil had been raised by a series of aunts and uncles who lived in a rural area of the Midwest. At age seventeen, he promptly joined the navy and spent the next four years traveling the world until he was honorably discharged at the age of twenty-two. He began drinking in the navy and continued throughout his adult life without any suggestion of problems for the next twenty years. Two failed marriages left him cautious about committing to any woman again even though he had a long string of short-term relationships over the last ten years. He worked for the airlines and his job required that he move every few years. Cecil showed up at a therapist office one day complaining of “ depression and lack of meaning in my life.” He quickly announced that he had gone to a few AA meetings since being transferred to the city and concluded he was an alcoholic. In fact, an AA member had given him the therapist’s name and had urged him to set up an appointment. Anti-depressants were promptly prescribed and Cecile agreed to enter an outpatient therapy group. During the course of the next few months Cecile religiously attended both AA and the group. With continual sobriety, he was able to identify a pattern to his drinking. “I never felt comfortable with my father or with men unless I was drinking with them.” He proceeded to paint a picture of a man who surrounded himself with “ drinking buddies” and “the locals’ tavern” became the one place where he felt he could count on “connecting with the regulars.”
Eventually, AA began to serve a very similar function to that of the “ local tavern”. He found a “ home group” and a bunch of men that he admired and looked up to. Cecile developed a relationship with a sponsor and began to faithfully work the steps of the AA program, frequently reading the “ big book” and “the daily meditations.” He admitted, “You know, I never did get into this god-thing that my aunts and uncles tried to force down my throat, but this ‘ higher power’ and ‘spirituality’ make sense to me.” A few months later, he excitingly announced to the group that a “ bunch of doctors and lawyers at the meeting invited me out to have coffee with them. They were asking me what they should do about working the steps. One of the lawyers even asked if I'd be his sponsor.
The Reparative Approach
In an attempt to explain the importance of self psychology as a treatment approach, Howard Bacal wrote, "One simply cannot apply unmodified classical drive theory in the clinical situation and expect that the patient will feel understood" (1992, p. 56). Bacal challenged the "considerable discrepancy between what effective classical theorists preach and what they practice."
His criticism has relevance because it is an attempt to bring classical psychodynamic theory in line with the practicalities of treating the addicted patient. Self-psychology helps accomplish this task because it offers a unique perspective, not only for addiction, but also for all psychopathology. Self-psychology departs from Freud's classical drive theory with its emphasis on intrapsychic conflicts and moves the focus of attention to relationships and the age-appropriate developmental needs that were unmet, which leads to arrested emotional development. Until this is repaired through the restoration of psychic structure, individuals will remain susceptible to seeking external sources of gratification because their internal self-structure is unable to provide this needed capacity.
Ormont (2001), writing from a modern analytic perspective, convincingly argued that since the developmental failures (parenting figures did not provide needed maturational input, creating a gap that leaves the child with developmental deficits in their personality) occurred before the maturation of language, pre-oedipal patients cannot respond to words or interpretations. Characterlogical change does not take place through interpretation, but through experience, “microinternalizations” of the therapist’s functions as a self-object. No further psychic growth, Ormont contends, is possible without these experiences.
Therapy, from this perspective, needs to be geared to the pre-oedipal patient’s developmental arrest, which left them with the inability to use feelings as signals and the incapacity to regulate their emotions. Developmentally arrested patients require a corrective emotional relationship to repair the deficit in their psychic structure. Therapy, from this perspective, takes on a goal very similar to the transformational experience that AA requires of its members if sobriety and recovery is to be achieved. Ormont (2001) writes about the importance of such a treatment approach.
“Like the child, the patient has a maturational need to internalize the admiration of a nourishing figure who derives pleasure from the pursuit of mastering challenges and overcoming obstacles. The child-patient has a need to merge with the idealized parent surrogate, to share in the security, standards, and calm of the analyst. The movement is from narcissistic need to a capacity to take care of oneself.” p. 345.
The Restoration of Healthy Self-Esteem
Healthy self-esteem is the end product of sufficient age-appropriate responsiveness and parental emotional attunement. Healthy parental role models provide the other necessary component of idealization that leads to healthy narcissism, which is basic to emotional health and consists of a subjective sense of well being and confidence in one's self-worth. A person who "feels" a balanced valuation of their importance and potential, and can relate in mature ways to others, will usually have a sense of meaning and know how they fit in the world.
In contrast to this, even though the majority of cocaine addicts and alcoholics appear to be very successful and are high achievers in their professional lives, those who work with these patients on a consistent basis are struck by how fragile their basic sense of self-worth has been. Despite their exaggerated striving for financial, physical, and intellectual success, their needs for approval and acceptance leave them consistently vulnerable to injury, rejection, shame, and humiliation.
"Individuals whose nascent selves have been insufficiently responded to will use any available stimuli to create a pseudo excitement in order to ward off the painful feeling of deadness that overtakes them" (Kohut and Wolfe, 1978, p. 418)
Healthy and Unhealthy Narcissism
Self psychology has consistently viewed healthy narcissism or mature narcissism as reflective not of the decrease of emotional investment in one's self but of a person's inability to establish mutually satisfying relationships with others in which giving and receiving are balanced. As Ornstien (1981) writes, "When... the self attains the capacity for becoming a relatively independent center of initiative... it is then also capable of recognizing the relatively independent center of initiative in the other" (p. 358). In the case of healthy narcissism, the person can hold a healthy respect for his or her uniqueness while, at the same time, being able to be in reciprocal resonance with the unique qualities and independence of another. Such a person can give as well as take and does not need to be one-up or one-down in a relationship.
In contrast, pathological narcissism requires either the presence of an idealized other (e.g. “My worth is enhanced by your power.”) or a mirroring self-object (e.g. “My worth is confirmed by your admiration of my power.”) in order for the afflicted individual to maintain narcissistic homeostasis. Self-objects in both categories occupy precarious positions, prone to devaluation or contempt if they should fail to provide their required functions. True reciprocal mutuality in a relationship is usually too taxing, overwhelming the narcissist’s capacity for acceptance of imperfections in self and other. Consequently, the give and take that is part of healthy mature relationships cannot be maintained.
Narcissism from this perspective ceases to be a source of healthy self-respect and self-esteem and becomes a defense—a “false self” or “grandiose self” that guards against painful feelings of shame and low self-worth. As Morrison (1989) convincingly demonstrated, shame or humiliation is always the underbelly or driving force behind a narcissistic defense. AA has long recognized that the alcoholic’s grandiosity or self-centeredness and lack of humility is the most important obstacle that has to be modified if sobriety is to be maintained. Using technically incorrect terms drawn from psychodynamic concepts, AA nevertheless captures the essence of the problem that must be addressed in recovery. Long before Kohut's theoretical formulations of grandiosity and narcissism, early pioneers in the treatment of alcoholism were writing of the necessity of "the surrender of the inflated ego” in an alcoholics' recovery. ( Tiebout, (1954). Bateson (1971) wrote that the biggest obstacle to an alcoholic’s recovery was a reluctance to relinquish "false pride". While the terminology may be different, the basic premise is similar. Early theorists recognized that narcissistic features, such as grandiosity, were a primary corollary in the addiction process.
False pride, inflated ego, and grandiosity are consequently viewed as defenses against feelings of inferiority and inadequacy. As Tiebout (1954) suggest, there has to be a reason why one has a need to inflate oneself. If an alcoholic or addict felt or believed they were enough, there would be no need for inflation of self or false pride. When individuals suffer from an absence of healthy self-esteem, they are left with an intolerable affect state often referred to as shame.
Morrison (1989) writes, ". . .the self’s experience of shame is so painful that the narcissistic constrictions of perfection, grandiosity, superiority, and self-sufficiency are generated to eliminate and deny shame itself... Shame, then, can be viewed as an inevitable feeling about the self for its narcissistic imperfection for failure, for being flawed" (p.66).
The cycle of remorse, shame, and self-loathing that subtance abusers experience the morning after a humiliating night of chemical abuse spurs them to make the false promises and vows to never let something like this happen again. Attempts at control inevitably fail, exacerbating the self-loathing and contributing to the rigidity of the defenses. Because of repeated failures, shame and remorse become intensified. The substance abuser is forced to combat the painful affect with his or her only available resources, namely, alcohol or drugs.
Khantzian (1994) holds the position that AA is corrective for the alcoholic because the program is able to penetrate the narcissistic defenses of false pride. The primary reason alcoholics suffer, according to Khantzian, is because they cannot control their drinking and they cannot control themselves. Unable to admit their vulnerabilities, they remain isolated, alone and cut off from others and themselves. What they need to do (admit their vulnerabilities to another), they cannot do because of the shame and their characterogical, grandiose, defensive posture. defensive posture. AA works because once initiation into the program occurs, contact with others is sustained, and through continued interaction with others, alcoholics are able to alter the dysfunctional interpersonal style that up to now has dominated their life. Kurtz (1982) and other interpreters of AA concur that shame that makes engagement and contact difficult, if not at times impossible, for many practicing alcoholics.
A New Definition for Addiction
The treatment of narcissism has many similarities to, and applications for, the treatment of addiction—especially if addiction is viewed as an epiphenomenon of narcissistic defenses against shame, fear, and other painful affect. Narcissism, like addiction, is a retreat into a grandiose-self or false-self personality organization as a way of avoiding the need for attachment. It results from unmet developmental needs, which leave certain individuals with an injured, enfeebled, uncohesive, or fragmented self. Vulnerable individuals are unable to regulate affect and in many cases are even unable to identify what it is they feel. Unable to draw on their own internal resources, they remain in constant need (object hunger) of self-regulating resources provided externally. Since painful, rejecting, and shaming relationships are the cause of their deficits in self, they cannot turn to others to get what they need or have never received. Deprivation of needs and object hunger leaves them with unrealistic and intolerable affects that are not only disturbing to others, but also shameful to themselves.
Consequently, addicted and alcoholic patients are always vulnerable to compulsive, obsessive, and addictive behavior, constantly substituting one addiction for another until the vulnerabilities in the self-structure are repaired and restored. Repair and restoration of the self can be accomplished only within a healing and healthy relationship. The patient needs a consistent, nurturing, mirroring, and holding environment that can contain and manage negative, destructive impulses while giving the patient the opportunity to identify, internalize, and incorporate a healthy set of introjects and internal object representations.
However, once the psychic structure is repaired and restored, it can be maintained only if, like any living organism, it is provided with an environment where it continually nurtured, fed, and allowed to flourish and grow. That can only be accomplished if substance abusers learn how to establish and maintain healthy intimate interpersonal relationships outside the therapeutic milieu. Since relationships can also become compulsive and addictive, substance abusers need to experience themselves in relation to others to fully understand how they contribute to their difficulties within the interpersonal sphere.
Self Psychology as a Deficit Theory
Some may have difficulty with the generalization and the lumping of all addictions under one category. An important aspect of any theory is its ability to identify and unite complex and seemingly unrelated phenomena into one simple truth. Self psychology and attachment theory accomplish this compellingly in the field of addiction. Kohut (1977) postulated that all addictions share an underlying similarity: they are all misguided attempts at affect-regulation and self-repair generated by inadequate psychic structure. Until psychic structure is built, the addict will have difficulty establishing intimate attachments and be inclined to substitute a vast array of obsessive-compulsive behaviors that serve as distractions from the gnawing emptiness that threatens to overtake them. Consequently, when one obsessive-compulsive type behavior is given up, another is likely to be substituted unless the deficiency in self- structure is corrected.
Vulnerability of the self is the consequence of developmental failures and early environmental deprivation. The absence of secure attachment leads to ineffective attachment styles, which persists through adulthood. Substance abuse, as a reparative attempt, exacerbates dysfunctional attachment styles because physical dependence and chemical use toxicity exacerbates the deterioration of existing physiological and psychological structures. Prolonged stress on existing structure leads to exaggerated difficulty in the regulation of affect, which leads to inadequate modulation of appropriate behavior, poor self-care, and rigidly ingrained patterns of object relatedness, which leads to increased character pathology. Kohut clarified the relationship between addiction and psychic deficits when he wrote:
"...the calming or stimulating effect which the addict obtains from the drug is.. ..impermanent. Whatever the chemical nature of the substance that is employed. ... No psychic structure is built, the defect in self remains. It is as if a person with a wide open gastric fistula were trying to still his hunger through eating. He may obtain pleasurable taste sensations by his frantic ingestion of food but, since the food does not enter that part of the digestive system where, it is absorbed into the organism, he continues to starve." (Kohut, p. viii, 1977)
The Self-Medication Hypothesis & Affect Regulation
Building on the early theoretical observations and formulations of Kohut (1977), Khantzian (1985) provides an alternative explanation for the addiction process that is not only compatible with the disease concept, but also expands it while providing useful and practical theoretical formulations that can enhance an addict's and alcoholic's treatment and recovery. The "self-medication hypothesis" has important implications for psychotherapy. It not only provides an explanation why substance abusers have a propensity to switch addictions, it also complements the way AA and other twelve-step programs treat chemical dependency.
In his earlier work with narcotic addicts, Khantzian (1982) first recognized that opiates were the drug of choice for certain individuals because of the drug’s specific pharmacological effects. Khantzian discovered that heroin addicts prize their drug for its anti-aggressive effects. It helped them soothe and calm their intense feeling of rage. He eventually discovered this to be similar for other drugs that reduce anxiety, depression, or other painful affect states. Chemically dependent individuals are in a sense acting as their own uncertified physicians to fix or repair what they are missing. Consequently, Khantzian hypothesized that it isn't pleasure so much that addicts are seeking; rather they are attempting to regulate their emotional selves and escape, even momentarily, from the constant feelings of deprivation, shame, and inadequacy that dominate their lives.
In his later work, Khantzian found that all substance abusers were predisposed to abuse or to becoming dependent on a particular drug because they suffered a particular impairment in affect regulation. He hypothesized that addicts were drawn to a certain drug because their 'drug of choice' matched their idiosyncratic deficits in regulating specific feelings. Although most addicts have experimented with many different drugs, they learn that a particular drug has a special appeal for them because of the drug's ability to regulate troublesome affect states. For instance, narcotic addicts are drawn to opiates because of its ability to relieve states of dysphoria associated with aggression, anger, and rage. Chronic depression, bi-polar illness, and hyperactive syndromes or attention deficit disorder (ADD) are symptoms highly represented in cocaine addicts. Addicts who felt bored, empty, dead inside, or that life was meaningless are frequently drawn to stimulants. Later experience showed Khantzian that counter-dependent, restricted, and inhibited individuals were likely to be drawn to alcohol and sedatives. Highly anxious and fearful people suffering from chronic anxiety are prone to use the benzodiazepines and likely to become dependent on minor tranquilizers like Valium and Zanax, while more isolated and schizoid individuals are attracted to marijuana and the hallucinogens. As Khantzian (1982) wrote, “this self-selection is related to the distinctive psychoactive actions of various drugs. ..in the course of experimenting with different drugs, an individual discovers that the action of one drug over another is preferred.” (p. 757).
The "self-medication hypothesis" has proved to have important implications for treatment even though many of its earliest assumptions have not been substantiated by later research. The recognition of the self-medicating function of abused substances helped shift the focus from a pleasure-seeking to a pain-relieving approach to understanding why alcoholics and addicts abuse substances. This shift enabled clinicians to engage in a more positive, compassionate psychotherapeutic relationship.
Affect Regulation Theory
Affect regulation theory carries with it the implication that everyone, not just addicts and alcoholics, need self-objects to help provide affect regulation. Certain individuals, because of genetic and environmental variables are more vulnerable to disruption because they suffer more severe deficits in this capacity. Vulnerable individuals are more dependent on outside sources or do not have the necessary interpersonal skills and to obtain regulation the way our species are geneticaaly hardwired to get it—through other people.
Because of Kohut’s and Khantzian’s persuasive reasoning, affect regulation theory helped shift psychoanalytic thinking about addiction from the more classic drive or instinct theory to the relational models (Guntrip, 1955; Fairbairn, 1952) with its greater emphasis on adaptation, developmental arrestment, and deficits in self-structure. Building on the early theoretical observations of Kohut (1977), Khantzian provided an alternative explanation for the addiction process that is not only compatible with the disease concept, but also expands it while providing useful and practical theoretical formulations that can enhance the substance abuser's recovery and treatment. Attachment theory, with its emphasis on the psychobiological aspects of the attachment experience helped legitimize many of the aspects of affect regulation theory. Both attachment theory and affect regulation theory challenged a formerly unspoken bias that dominates our culture and the mental health model: dependency is bad.
Dependency & Pathology
Bowlby cautioned therapists about their tendency to confuse healthy attachment needs with dependency. Too often, clinicians use the term attachment to explain adult pathology (West & Sheldon-Keller, 1994). A person’s need for reassurance, comfort, and understanding, especially during times of distress, must not be construed as pathological or as a regression to immature behavior, especially when someone is threatened by loss. Many therapists are too quick to impose these views or agree with a patient’s self-assessment when the patient admits with embarrassment that they are “too needy.” These value judgments are built into the idea of dependency. They are often reflected in a therapist’s appraisal, which are reinforced by a culture that equates independency with maturity and mental health. In the rush to combat the demon of dependency, patients are often re-traumatized, feeling much as they did when their critical parents shamed them for seeking comfort or assurance.
To be dependent on someone is not the same as being attached. Attachment is an emotional bond that forms over time with care-giving, familiarity, and continuity. Someone can be attached and not dependent. Consequently, it is also possible to be dependent and not attached, which is what co-dependency is all about. As attachment theory implies, dependency is not only a confusing and pejorative term, but reflects a strong bias in our culture that not only reflects our obsession with autonomy and independence at all costs, but also is not in line with the biological realities of our species.
Critics of AA (i.e. Tournier, 1979; Jones, 1970) often express concern that the addict and alcoholic may become too dependent on the program and they judge the alcoholic’s reliance on AA with concern and suspiciousness. Even if one accepted the premise of this argument, isn’t it preferable to have a dependence on an organization that promotes health, sobriety and helping others over a drug that promotes sickness, death and immeasurable suffering to oneself, family and society. For some reason, many professionals fail to understand how their devotion to their church, tennis club or professional organization is any less dependent than an AA member's devotion to AA.
Weinbergh (1975) expresses similar sentiments when he writes, “Even if one accepted the premise (which to be consistent would also seem to rule out devotion to an organized religion or to psychiatric cults such as psychoanalysis), the author is hard pressed to consider this argument as reasonable. Since one cannot deny that alcohol dependency is extremely harmful to the individual, his family, and society, whereas AA dependency means sobriety, stability, and helping others as a result of living the program, what is the alleged harm in substituting the latter for the former?” (p. 34.)
AA members are in fact told, "You did not get sober to go to AA meetings.” Dependency is actually discouraged in the program. What often gets passed off as dependency by AA's critics is actually the alcoholic's investment of himself in relationships within the AA fellowship. Often, this is the first time that the AA member has engaged in any type of meaningful human contact while not drinking or intoxicated.
It is unfortunate that so many professionals view it as a negative turn of events. A common suggestion is to get the addict or alcoholic to "face the world as it really is." In contrast to the accusations that suggest AA fosters pathological dependency by substituting one dependency for another, is the consideration that the emergence of such dependent behavior actually signals an important change in a positive direction. Such an occurrence is often the first evidence of the alcoholics' ability to engage in one-to-one relationships, which allows them to accept their need for help and to find new people with whom they can identify. This process takes time. If this process is not interrupted, the addicted individual will eventually develop a healthy capacity for mutuality and secure attachment.
Closely related to this principle of healthy dependence on others is the maturation of narcissistic needs for self-objects and affect regulation. Kohut differentiated between archaic needs for self-objects (which is a reparative process that involves the building of psychic structure) and mature needs for self-object responsiveness (which involves the mutual regulatory process that goes on between two healthy individuals who provide the type of regulation that keeps each other functioning at a optimal level). Early in recovery, alcoholics and addicts typically need archaic self-objects. Their reliance on the excessive use of grandiose defenses is intertwined within the fabric of values expressed by the drug and alcohol subculture. Recovery and abstinence interfere with the narcissistic fixations of their chemical using lifestyle. Treatment works best when it provides a course for recovery that facilitates the maturation of healthy narcissism. Sometimes, this may required the individual develop an idealized attachment to the program.
An idealized attachment to a program allows an individual's narcissistic needs to be met in a healthy fashion. It can be reparative experience if the substance abuser internalizes the admired values expressed in the philosophy of the program. Since AA values are often enthusiastically held by its members, they represent a direct confrontation with the tenets held by the drug and alcohol subcultures. By idealizing the values of the AA program, alcoholics and addicts not only become less enamored with drinking and drug use, they also develop an healthy dependence upon those they idealize.
Self-object Transferences: Implications for Treatment
As a result of insufficient self-object responsiveness, the substance abuser lacks self-worth and suffers from chronic feelings of poor self-esteem and shame. It is within the matrix of environmental responsiveness and emotional attunement that a specific process of psychological structure formation develops. Structure building cannot occur without a previous stage in which the child's mirroring, twinship, and idealizing needs have been responded to efficiently. Structure is laid as the consequence of minor, non-traumatic failures in the responses of empathic self-objects. Specifically, structure is built when the ruptured bonds between the self and the person providing self-object functions is restored (Harwood, 1998). Resolving disagreements in an ideal atmosphere of optimal frustration permits the self to gradually internalize the functions previously provided by the self-object. Optimal frustration reflects the ideal environmental situation within which these minor, non-traumatic failures occur.
Empathic failures, within the context of optimal frustration, leads to a gradual replacement of the self object functions by the individual's developing capacity to soothe and calm oneself. Kohut called this process transmuting internalization. If affect- regulation and self-soothing are internalized, the person will be less dependent on external sources for gratification. The more the holding environment provides opportunities for empathic failures to be worked through and repaired, the greater the frequency that ruptured bonds with the caretaker will be re-established and, subsequently, the stronger the structure formation will be (Beebe, 1993).
Clinical Example
Dorothy was more than two years sober and active in AA when her female therapist referred her to a mixed group of men and women to give her “an opportunity to work on her issues with men”. The only sister in a family with four brothers and a father who was a major in the air force, Dorothy was the constant recipient of ridicule and mockery. Since the group was co-led by a man and a woman, Dorothy was able to align herself with the women in the group and use them as a buffer as she dealt with her male siblings in the group. However, her biggest challenge came from her dealings with the male leader. Any failures, imagined or real, on his part to defend or understand her were met with emotional storms of protest and outrage. With the group, and especially the women, serving as a bulwark against overwhelming fears of retaliation, Dorothy received the encouragement and support she required in order to work through all injuries as they occurred. With the male therapist’s consistent patience, each repair allowed psychic structure to be established, providing her with a greater capacity to not only stand up for herself, but to tolerate shortcomings in men without viciously attacking them.
Psychic structure, from a self psychology perspective, is not an entity or an agent, but a capacity, indicating a class of psychological functions pertaining to the maintenance, restoration, and consolidation of self-experience. Psychic or self-structure represents the capacity or ability to integrate and organize fragmenting affect into meaningful experience. Structure formation—the acquisition of patterns and meaning—is developed out of the internalization of functions previously provided by external objects and reflects the ability to take over these functions without relying excessively on self-objects. The deficits in psychic or self-structure that require external augmentation are usually the result of developmental failures related to unmet age-appropriate attachment needs. Conversely, the successful formation and establishment of self-structure is a developmental outcome reflecting the capacity for affect regulation.
In treatment, optimal frustration should not be confused with deliberate attempts on the therapist's part to frustrate the patient. Frustration naturally occurs in any genuine ongoing relationship. Optimal refers to the climate established in the holding environment which most favorably allows for the re-establishment of ruptured bonds in an atmosphere of optimal responsiveness. If a proper treatment environment is created, structure formation will be the natural by-product of the spontaneous interactions that occur within the therapy relationship.
Parallels Between Psychic Structure & Internal Working Models
There exists a complimentary relationship between Kohut’s definition of psychic structure and Bowlby’s internal working model. Following Kohut's work on self object transferences, substance abusers are viewed as having been deprived of the opportunity to adequately internalize the admiring, encouraging, valued, and idealized qualities of good enough parental figures. Absence of this experience inhibits further developmental growth, interfering with the gradual internalization of the self-object function. Until these capacities become internalized, the vulnerable individual—through the force of the repetition compulsion—willcontinue to recreate their past in the present. Attachments to external bad objects (i.e., a cold, critical mother, drugs, alcohol, etc.) in the external world are extremely difficult to relinquish until internalized object and self-representations are worked through, modified or altered. Ogden writes, “resistance is understood in terms of the difficulty the patient has in giving up the pathological attachments involved in his unconscious internal object relations. ...This tie is based on one's need to change the bad object into the kind of person one wishes the object were... The second category of the bond to a bad internal object... takes the form of a crusade to expose the unfairness of, coldness of, or other forms of wrong doing on the part of the internal object.” (1983, p. 236)
The attachment to the tantalizing, internalized, split-off, good object and self-representations is the collected bond that fuels the addictive process. The needy but undeserving good self-representation is not only a bottomless pit that can never be satisfied, but the tantalizing good object can never fulfill its promise of perfect love, acceptance, and complete nurturance without any limits or disappointments. The overindulgent, over-gratifying, and inconsistent mother can be as damaging to the child's development as the cold, critical, and rejecting mother. In the former case, frustration tolerance is never internalized and impulse control is never mastered. Ogden writes, “one type of tie to a bad internal object is the attachment of the craving self to the tantalizing object. The nature of the tie to the object is that of the addict for the addicting agent and is extremely difficult to relinquish.” (1983, p. 236)
Disturbances in attachment during the formative years of development increase the potential for psychopathology and establish an “internal working model” which impacts future attachment styles. In a similar fashion, attachment-oriented therapy can be defined as a way of eliciting, exploring, integrating, and modifying internal working models. It is helpful to think of all interpersonal interactions as operating on two levels. There are the observable interchanges occurring between individuals in the external world and the internal exchanges of self and object representations occurring within each person’s internal working model. Each level of interaction influences the other. Just as a person’s external behavior is modified by interactions with others, adaptations in internal self and object representations are also occurring. This approach to treatment operates on the principle that internal structural change is necessary if external behavioral change is to be long lasting.
The Lifelong Need For SeIfobjects & Affect Regulation
Bowlby saw the need for healthy relationships that provided mutual affect regulation as an integral part of human behavior “from the cradle to the grave” (1988). Kohut agreed and said that we never outgrow our need for self- objects and that therapy is only complete when the person can form healthy attachments outside of the therapeutic milieu. Both attachment theory and self psychology view the disease concept as a metaphor and provide alternative explanations why AA works and why abstinence is required. However, as attachment theory reminds us, regardless of our age or emotional development, we will always require some degree of emotional regulation from others. The denial of the need for others is what leads individuals to seek gratification (i.e. drugs, alcohol, food, sex, work, gambling, etc.) outside the realm of interpersonal relationships.
AA & Narcissism
Kohut viewed the narcissistic disorder as the expression of a reaction to injury of the self and regarded the experience of the bond between the self and the self object to be crucial for psychological health and growth. Kohut is implying that there is an inverse relationship between individuals' early experience of positive self-object responsiveness and their propensity to turn to alcohol, drugs, and other sources of gratification as substitutes for these missing or damaging relationships. Conversely, if they are to successfully give up these misguided attempts at self-repair, they must learn how to substitute healthy interpersonal relationships in which needs for self-object responsiveness (mirroring, merger, and idealization) are satisfied in a gradual, gratifying way.
AA and other twelve-step programs provide a predictable and consistent holding environment that allows addicts and alcoholics to have their self-object needs met in a way that is not exploitive, destructive, or shameful. Because of unmet development needs, addicts or alcoholics have such strong and overpowering needs (object hunger) for human responsiveness that they feel insatiable and shamed by their neediness. Through their identification with other alcoholics and addicts, they come to accept in themselves what they could not previously because they believed their badness was unique.
Addicts or alcoholics can only tolerate acceptance at this level of emotional vulnerability because they feel understood on a very basic, empathic level. Empathy and emotional attunement are not only the corner-stone of treatment for self-psychology, they are also the foundation from which chemically dependent individuals can begin to feel the kind of responsiveness and gratification they had been missing and were previously unable to tolerate in their lives.
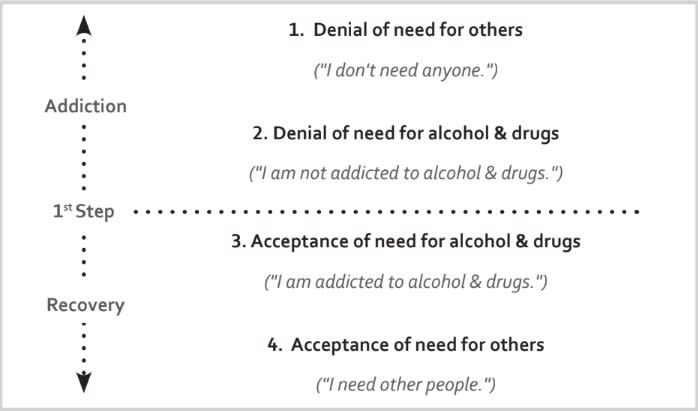
As Kurtz (1979) has eloquently argued in his book, Not God, alcoholics must come to terms with their narcissistic defenses and quit playing God. Kurtz writes, “Not-God” means first “You are not God”, the message of the AA program . . . The fundamental and first message of Alcoholics Anonymous to its members is that they are not infinite, not absolute, not God. Every alcoholic’s problem had first been, according to this insight, claiming God-like powers, especially that of control. But the alcoholic at least, the message insists, is not in control, even of himself: and the first step towards recovery from alcoholism must be the admission and acceptance of this fact that is so blatantly obvious to others but so tenaciously denied by the obsessive-compulsive drinker.” P.42.
The next illustration sums up Kurtz’s position. Parallel to attachment theory and self psychology, Kurtz says it is the alcoholic’s denial of his need for people that leads to his eventual denial that he is an alcoholic. Consequently, recovery is dictated by reversing this process. First, the alcoholic must admit that he is an alcoholic and then he must ultimately admit he needs people.
In an existential sense, the confrontation between what the substance abuser tried to be and what they really are (not-God) results in them ceasing to live their life in bad faith (i.e. alcoholic) and become more authentic ("Hello, I'm Joe, a recovering alcoholic") with all the limitations that authentic life imposes on them. As archaic ways of getting one's needs met are gradually relinquished for more mature ways of establishing close human contact (removal of character defect by working the program), the alcoholic or addict is able to internalize more self-care and monitoring of affective states (transmuting internalization). The central issue in this process is the acceptance of one's self as one is, which requires dealing with shame about the self that was previously hidden.
AA, as a holding environment, also becomes a transitional object; a healthy dependency that provides enough separation to prevent depending too much on any single person until individuation and internalization are established. Gradually, alcoholics or addicts are able to give up the grandiose defenses (narcissism) and false-self persona for a discovery of self (true self). As David Treadway (1990) points out, the self-help movement is, regardless of its successes or failures, driven by people’s attempts to regain the “lost spirit of community.”
This article is adapted from, Addiction as an Attachment Disorder by Philip J. Flores (2004). Adapted by kind permission of Jason Aronson, Inc. A Member of The Rowman & Littlefield Publishing Group, Inc Lanham, Maryland, 20706.
AA References
Alcoholics Anonymous. (1939). Alcoholics Anonymous. New York: AA World Services.
Bacal, H. A. (1985) ‘Optimal responsiveness and the therapeutic process.’ In A. Goldberg (ed) Progress in Self Psychology. New York: Guilford Press, pp. 202-226.
Bacal, H. A. )1992). Contributions from self-psychology. In R. Klien, H. S. Bernard, & D. L. Singer (Eds), Handbook of group psychotherapy (55-86). Madison, CT: International University Press.
Barber, J. P., Luborsky, L., Critis-Christoph, P., Thase, M. E., Weiss, R., Frank, A., Onken, L., & Gallop, R. (1999). Therapeutic alliance as predictor of outcome in treatment of cocaine dependence. Psychotherapy Research, 9, 54-73.
Bateson, G. (1971). The cybernetics of self: A theory of alcoholism. Psychiatry, 34, 1-18.
Beebee, B. (1993) ‘Contributions from Infant research.’ Film shown at the 16th Annual Conference on the Psychology of the Self. Toronto, Canada, October, 1993.
Bowlby, J. (1973) Attachment and loss: Vol. 2. Seperation: Anxiety and anger. New York: Basic Books
Bowlby, J. (1979) The making and breaking of affectional bonds. London & New York: Routledge.
Bowlby, J. (1980). Loss: Sadness and Depression. New York: Basic Books.
Bowlby, J. (1988) A Secure Base. Clinical Applications of Attachment Theory. London: Routledge.
Fairbairn, W. R. D. (1952) Psychoanalytic studies of the personality. London: Routledge & Kegan Paul.
Guntrip, H. (1974). Schizoid Phenomena, Object Relations and the Self. London. Hogarth Press.
James, W. (1902). The varieties of religious experience. New York: Longmans.
Jones, R. K. (1970). Sectarian characteristics of Alcoholics Anonymous. Sociology, 4, 181- 195.
Khantzian, E. J. (1982). Psychopathology, psychodynamics & alcoholism. In E. M. Pattison & S. E. Kaufman (Eds.), Encyclopedic handbook of alcoholism (581- 597). New York: Gardner Press.
Khantzian, E. J. (1985). On the psychological predisposition for opiate & stimulant dependence. Psychiatry Letter, 3(1), 1-3.
Khantzian, E. J. (1994). Alcoholics Anonymous—Cult or corrective? Paper presented at Fourth Annual Distinguished Lecture. Manhasset,. NY: Cornell University.
Khantzian, E. J. (1999). An Interview with Dr. Edward J. Khantzian. In Psychotherapy Book News, July 29, 1999, 8-13.
Khantzian, E. J. (2001). Reflections on Group Treatments as Corrective Experiences for Addictive Vulnerability. International Journal of Group Psychotherapy, 51, 11-20.
Khantzian, E. J., Halliday, K. S., & McAuliffe, W. E. (l990). Addiction and the vulnerable self. New York: Guilford Press.
Kohut, H. (1972). ‘Thoughts on narcissism and narcissitic rage.’ Psychoanalytic Study of the Child. 27, 360-400.
Kohut, H. (1977) Preface in J. D. Blaine & A. D. Julius (Eds), Psychodynamics of drug dependence. NIDA Publication No. ADM 77-470. Washington, D C: Superintendent of Documents, U.S. Government Printing Office.
Kohut, H. (1978) Creativeness, charisma, group psychotherapy. In P. Ornstien (ed) The Search for the self (Vol.2). New York: International Universities Press.
Kohut, H. (1982) Introspection, empathy, and the semi-circle of mental health. International Journal of Psychoanalysis, 63, 395-407.
Kohut, H. (1984) How does analysis cure?Chicago: University of Chicago Press.
Kohut, H. & Wolfe, E. S. (1978). The disorders of the self and their treatment: An outline. International Journal of Psychoanalysis, 60, 413-424.
Kosseff, J. W. (1975). The leader using object-relations theory. In Z. A. Liff (Ed.), The leader in group (212-242). New York: Jason Aronson.
Kurtz, E. (1979). Not-God: A history of Alcoholics Anonymous. Center City, MN: Hazelden.
Kurtz, E.(1982). Why A.A. Works. The intellectual significance of Alcoholics Anonymous. Journal of Studies on Alcohol, 43, 38-80.
Lewis, T., Amini, F., & Landon, R. (2000) A general theory of love. New York: Random House.
Lieberman, M. A. & Borman, L. D. (1979). Self-help groups for coping and crisis: Origins, members, processes & impact. San Francisco: Jossey-Bass.
McKeller, J., Stewart, E. & Humphreys, K.(2009). Alcoholics Anonymous Involvement & Positive Alcohol-Related Outcomes: Cause, Consequence, or Just a Correlate? A Prospective 2-Year Study of 2,319 Alcohol-Dependent Men. Journal of Counseling & Clinical Psychology, Vol 71, No. 2, 3002-3008.
Miller, M. S. (1995). Treatment of addictions: Applications of outcome research for clinical management. Binghamton, N. Y.: Haworth Press.
Morrison, A. P. (1989). Shame: The underside of narcissism. Hillsdale, NJ: Analytic Press.
Ogden, T. H. (1983). The concept of internal object relations. International Journal of Psychoanalysis, 64, 227-241.
Ormont, L. (2001) Meeting Maturational Needs in the Group Setting. International Journal of Group Psychotherapy. 51, 343-360.
Ornstein, P. (1981). The bipolar self in the psychoanalytic treatment process. Clinical & theoretical considerations. Journal of American Psychoanalytic Association, 29, 353-375.
Ornstein, P. (1982). Self Psychology. Lecture Series: University of Cincinnati, January-March, 1982.
Project MATCH Research Group. (1997). Matching alcoholism treatments to client heterogeneity: Project MATCH post-treatment drinking outcomes. Journal of Studies on Alcohol. 58. 7-29.
Stolorow, R. Brandchaft, B. and Atwood, G. (1987) Psychoanalytic treatment: An intersubjective approach. Hillsdale, NJ: Analytic Press.
Stone, W. N. (1992). The place of self psychology in group psychotherapy: A status report. International Journal of Group Psychotherapy, 42, 335-350.
Sullivan, H. S. (1953). The interpersonal theory of psychiatry. New York: W. W. Norton.
Tiebout, H. M. (1954). The ego factors in surrender in alcoholism. Quarterly Journal of Studies on Alcohol. 15, 610-621.
Tournier, R. E. (1979). Alcoholics Anonymous as treatment and as ideology. Quarterly Journal of Studies on Alcohol, 40. 230-239.
Treadway, D. (1990). Codependency: Disease, metaphor, or fad? Family Therapy Networker, 14(1), 38-42.
Weinberg, J. R. (1975). A.A.: An Interpretation for the Non-believer. Center City, MN: Hazelden.
West, M. L. & Sheldon-Keller, A. E. (1994). Patterns of Relating: An Adult Attachment Perspective. New York: Guilford.
Winnicott, D. W. (1965), The Maturational Process and the Facilitating Environment. New York: International Press.
Wolf, E. S. (1985). The search for confirmation: technical aspects of mirroring. Psychoanalytic Inquiry 5: 271-282.
Wolf, E. S. (1988) Treating the Self: Elements of Clinical Psychology. New York and London: The Guilford Press.
Philip J. Flores, Ph.D, ABPP, CGP, FAGPA is a clinical psychologist who is in private practice in Atlanta, Georgia.
Important: TherapyRoute does not provide medical advice. All content is for informational purposes and cannot replace consulting a healthcare professional. If you face an emergency, please contact a local emergency service. For immediate emotional support, consider contacting a local helpline.
Find Therapists
Must Read
Creating Space for Growth: How Boundaries Strengthen Relationships
Setting healthy boundaries fosters respect, protects emotional well-being, and strengthens relationships by defining personal limits and maintaining self-care.
International Mutual Recognition Agreements for Mental Health Professionals
Mutual recognition agreements for mental health professions are rare and uneven, with major gaps in counselling, social work, and allied therapies. Read on to understand ...
Jumping to Conclusions
Jumping to conclusions is a thinking habit where we assume the worst or make judgments without enough evidence. By recognising this pattern, therapy can help you slow dow...
Case Conceptualisation
Case conceptualisation is how a therapist thoughtfully pulls together your concerns, experiences, and strengths into a clear understanding of what’s going on. This shared...
Guided Discovery
Guided discovery invites clients to arrive at their own insights through collaborative questioning and reflection. Instead of being told what to think, individuals learn ...
About The Author

New Therapist Magazine
Pietermaritzburg, South Africa
“An independent, subscription-based magazine for mental health therapists, produced by journalists and therapists on five continents.”
New Therapist Magazine is based in Clarendon, Pietermaritzburg, South Africa.
