
Dreams: Theory and Clinical Practice- Part 2

❝A brief history of dreams in EARLY psychoanalytic thinking.❞
As you may know psychoanalysis and dream interpretation were co-creations, joined at the hip. It was in 1900 that Freud published his Interpretation of Dreams, a book which, despite its formidable length and Germanic heaviness, contains many of Freud’s core discoveries of mind: the existence of unconscious ideation, the pleasure principle, the reality principle, psychic dynamism and the value of free association to unmask disguised unconscious ideas and wishes. Just to be clear, and in case you are unfamiliar with these terms, some definitions are relevant here:
1. Unconscious ideation meant for Freud, not just that which is out of mind at a particular moment of time, but material which, without considerable mental work, remains permanently out of awareness. I am prepared to argue the point, but it now seems inescapable that our earliest wishes, memories and fantasies, actively effect our everyday decisions and behaviors while themselves remaining stubbornly in the shadows.
Looking for evidence-based support? Find a qualified psychologist near you through TherapyRoute.
Find a Psychologist2. The Pleasure Principle, among Freud’s psychoanalytic concepts, refers to Freud’s assumption that the primary aim of every human act, including mentation itself, is to obtain the maximal available gratification from any given situation. The phrase that captures this urgency best is: “I want what I want, whenever I want it and I want it NOW!” This is the earliest form of “thinking-wishing;” Freud labelled it the Primary Process. In its purest form it is characterized by a denial of time, logic, or external reality in its search for the quickest gratification of any impulse. We will see later that this kind of thinking: mobile, illogical, symbolic, fluid, is what dominates dream life, the playground, par excellence, of the eternal child who exists within us all.
3. The Reality Principle is, as it implies, the gradual awareness that the immediate effort to gratify certain wishes could be cataclysmic to the organism. Acceptance of the limits of the external world leads to rational thought, what Freud labelled The Secondary Process, and adult rational “planning.” Maturation and mental development itself is seen by psychoanalysts as the outcome of the inevitable clash of an immediate wish coming up against the exigencies of an increasingly complex and dangerous outside world. As a gross example: the baby at one year is hungry, he cries out and mother comes with breast or bottle. The “baby” at 13 is hungry, realizes he is too old to cry, appreciates that mother no longer comes anyway, decides to make himself a sandwich and hopefully, over time, gradually comes to realize the value of a regular income and a steady job to provide for his needs.
4. Psychic dynamism implies that cause and effect are forever active in the mind. Ideas are almost always related; thus, if one idea follows another, no matter how seemingly disconnected and distant they may appear, psychoanalysts assume a conscious or unconscious connection between those ideas. Having practiced for more than thirty years, I am still amazed at the degree to which remarks, seemingly miles from each other, upon careful ideational and emotional exploration, are discovered to be psychically intertwined in the mind of the utterer.
5. Free Association is a technique that replaced hypnosis and capitalizes on the ubiquity of the above referenced: psychic dynamism. Thus, a psychoanalyst by encouraging his patient to “just ramble on,” can feel confident that, in doing so, the patient will unwittingly communicate the full panoply of his desires embedded in the multitude of symbolic and real forms open to his mind.
Freud’s early and formative exposure to post-hypnotic suggestion with Jean-Martin Charcot at the Salpetiere, convinced him that patients “knew” a great deal more of their conflicts than they thought they did. Important pathogenic memories existed in a state which at one moment seemed absent, but under the right conditions, whether hypnosis or the pressure of his hand on their forehead while lying on a couch, could be recovered. Freud posited that these memories were stored in a particular part of the mind he called the Pre-conscious, a region which he theorized was bordered on one side by our conscious minds and on the other a region of ever more unrecoverable mentation which he labelled The Unconscious.
The Topographic Model
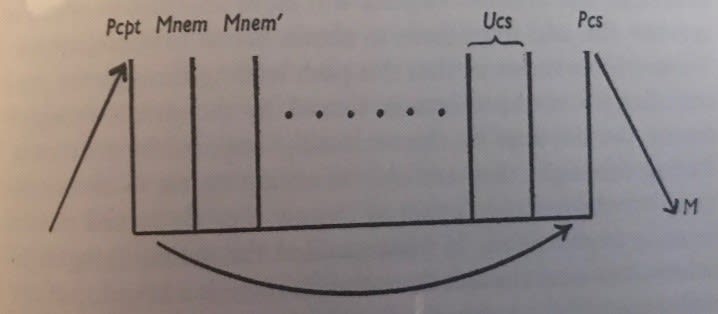
This is Freud’s first model of the mind: the so-called Topographic Model. A stimulus arising from the sensory (input) side, whether from within or outside of the body disturbs the prevailing homeostasis, impinges on the mind and forces the mind to “do something”. There is normally some slight delay before the individual performs an action intended to “solve” his problem. The delay between the stimulus and activation of the motor endplate constitutes “thinking.” Note that this model implies a movement forward in time not just from stimulus to motor behavior but also as the patient accesses his earliest memories forward to conceive of and create an “action plan.”
Recovery of memories from infantile amnesia led Freud to assume that the earliest of experiences, stimulus, fantasy and outcomes, were immortalized somewhere at the base of the Unconscious. While banished from conscious awareness, these unconscious trends, or, as neuroscientist Mark Solms likes to call them, these emergency “plans,” are always ready at hand to make sense of any new circumstance and offer a method of “handling” the current situation.
I don’t wish to belabor all this but there are at least two important aspects of mental life considerably clarified by this model. You will note that at the boundary of the pre-conscious and the unconscious there is a required “transfer” of meaning from the earliest experiences and memories of life, which are unavailable to consciousness, to that which is currently being attended to in the permeable pre-conscious. You might think of George Washington’s need to cross the Delaware River to engage the British.
This is the original meaning of the term “transference” which later became so closely associated with psychoanalytic and psychodynamic work. As initially conceived, it was merely the requirement that such a “transfer” take place at the border between these regions allowing an idea or feeling from the deepest past to reach the preconscious and through it, to gain access to consciousness. Such a process inherently required the use of simile, metaphor or implied metaphor; in other words, some internal assessment that: “This situation is or seems to be just like this other situation.”
Because Freud’s first model of the mind was based on the capability of an idea to reach consciousness, a transference of meaning was required; but you can readily see how the term was generalized and adapted to describe current relationships, including that with the therapist, which appear to reflect the consequence of a similar “transference” e.g. the putting into action one of those early unconscious “plans.”
As an aside I would remind you of a number of terms analysts previously used to identify what they felt was an optimal analytic stance, but which came to be viewed quite negatively in the larger treating community. These included suggestions about the need for “silence and neutrality” or the metaphor of being like a “blank screen” or adopting the attitude of a cold “mental surgeon.” These recommendations were not promoted because psychoanalysts are or were inherently rude, asocial or cruel, though in individual instances that might well be the case, but because, the presence and nature of transference distortions were felt to become ever clearer and therapeutically available for interpretation if one was working with a therapist whose personal life is largely unknown.
To return to the Topographic Model for a moment, Freud’s initial effort has been likened to looking through a spyglass from the opposite end in that it looks backward in time to the very earliest of memories and experiences. This model underscores that the creation of a dream implies a regression both structurally and in time, as the dream, barred from access to the motor endplate, turns backward touching on ever earlier material to end finally as a sensory experience .
Freud understood the dream as the earliest of responses to a disturbing stimulus and proposed that initially such a disturbance was and could be extinguished simply via hallucination.
One of the central requirements for every newborn infant is rest and sleep. The extinguishing of the bothersome stimulus to allow for added sleep Freud posited as the very first “emergency plan.”
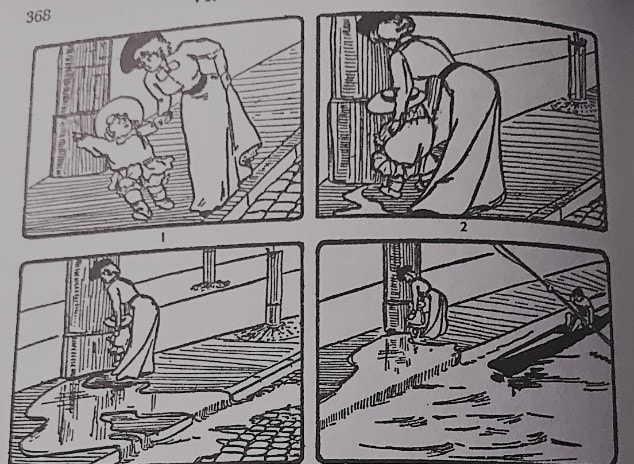
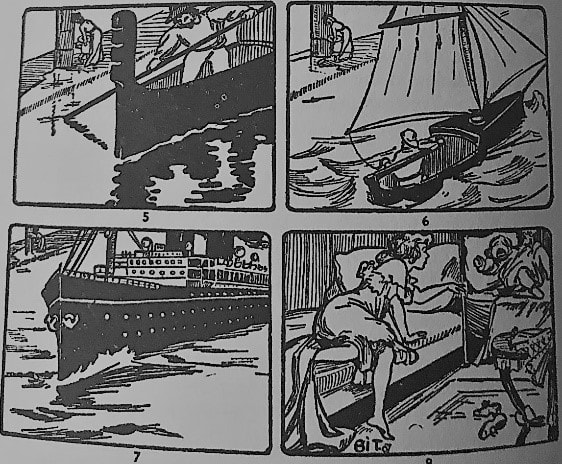
Note the dream portrayed above. The little boy begins to urinate, first a stream, then a creek, a river, an ocean and it is only then, with the dream failing to contain the “stimulus” that the parties awake.
Interestingly, this dream entitled the French Caretaker could “work” for both the baby and his caretaker; since these images would allow both the pleasure of additional time asleep, the baby by transiently ignoring the pressure of his bladder, the nurse by ignoring the increasing noise attending the baby’s
Whereas the Topographic Model has long been superseded, it does offer an intriguing explanation as to why language and rational thinking would be largely absent from dream life and further, that on its way to a hallucination of satisfaction, like a magnet passing over iron filings, the dream would draw on ever earlier versions of relationships and wishes of life. It was for this reason that Freud was to claim that embedded in every dream is an “infantile scene.” Freud was convinced that if one could find the inciting element of a neurosis, emotional catharsis and explication of that infantile situation could cure or vastly diminish neurotic trends. Thus, he afforded a special place for dreams seen as the “royal road” back to, as it were, the seat of the action or, as he liked to put it: “the source of the Nile.”
Douglas J. Van der Heide, M.D. is a training and supervising psychoanalyst at the Psychoanalytic Association of New York affiliated with New York University Medical Center and a member of the New York Psychoanalytic Institute
Navigation Menu
Part One:
Why dreams?
Part Two:
A brief history of dreams in EARLY psychoanalytic thinking.
Part Three: Important shifts in the psychoanalytic understanding of the nature of dreams and “dream-thoughts.”
Part Four:
How a composite understanding of dreams can be used by therapists in their daily work.
Photo by Jr Korpa on Unsplash
Important: TherapyRoute does not provide medical advice. All content is for informational purposes and cannot replace consulting a healthcare professional. If you face an emergency, please contact a local emergency service. For immediate emotional support, consider contacting a local helpline.
Find Therapists
Must Read
Creating Space for Growth: How Boundaries Strengthen Relationships
Setting healthy boundaries fosters respect, protects emotional well-being, and strengthens relationships by defining personal limits and maintaining self-care.
International Mutual Recognition Agreements for Mental Health Professionals
Mutual recognition agreements for mental health professions are rare and uneven, with major gaps in counselling, social work, and allied therapies. Read on to understand ...
Jumping to Conclusions
Jumping to conclusions is a thinking habit where we assume the worst or make judgments without enough evidence. By recognising this pattern, therapy can help you slow dow...
Case Conceptualisation
Case conceptualisation is how a therapist thoughtfully pulls together your concerns, experiences, and strengths into a clear understanding of what’s going on. This shared...
Guided Discovery
Guided discovery invites clients to arrive at their own insights through collaborative questioning and reflection. Instead of being told what to think, individuals learn ...
About The Author

“I am a highly trained psychoanalyst and my work is primarily with resolution of unconscious repetition of emotional conflict.”
Douglas Van der Heide is a qualified Psychiatrist, based in New York, United States. With a commitment to mental health, Douglas provides Assessment, Psychiatry, Individual Therapy and Online Therapy.



